Background: The essential elements of physicians’ daily practice occur within the clinical learning and working environment (LWE), the crossroads where medical education and lifelong learning intersect with direct patient care. The LWE, therefore, is the keystone for academic hospitalists interacting with learners across the medical education continuum. It is of equal significance for direct-care hospitalists who also continuously expand their knowledge and may teach non-physician colleagues and interprofessional learners. National drivers in hospital medicine including work compression, throughput pressures, patient complexity, etc. threaten the quality of the LWE. To navigate these pressures successfully, those seeking to optimize the LWE must start with a shared reference point from which to approach improvement in a comprehensive fashion. A recently published conceptual model enables this shared mental model and fosters a systematic approach to optimizing the LWE. The Learning and Working Environment is the nesting of personal, relational, curricular, and structural domains as traversed by multiple learners, centered on the needs of individuals or populations of patients, and influenced by the sociocultural context (Figure 1). This model can be utilized as a systems-based framework to address challenges across the continuum of hospital medicine – university/community hospital, observation unit, general inpatient ward.
Purpose: Hospitalists at three institutions across the country applied the LWE conceptual model to develop innovations specific to the field of hospital medicine and to their unique clinical circumstances. In describing these programs, this innovation abstract builds upon prior published work that presented the conceptual model and provided exemplar use-cases. Here, we describe concrete examples of effective utilization of the LWE conceptual model framework in hospital medicine settings.
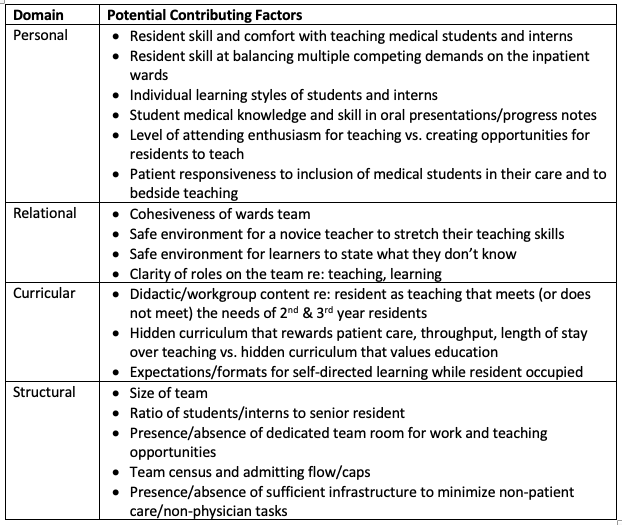
Description: One hospital medicine division recognized a need to enhance their Resident as Educator program after noting that residents on the inpatient ward service feel a tension between patient care duties and efforts to teach interns and students. Through application of the LWE conceptual model, contributing factors within each of the domains were identified (Table 1). By exploring each of these areas and determining their relative impact, academic hospitalist leaders successfully developed a pilot program to enrich the Resident as Educator program in a comprehensive way.Two additional examples of practical application of the LWE conceptual model in hospital medicine divisions across the country will also be described:1. Improving the care of patients with opiate use disorder by optimizing the hospital medicine LWE2. Addressing hospitalist physician mistreatment by patients or family members.
Conclusions: The clinical Learning and Working Environment (LWE) is a complex system, and as such, it requires a conceptual model that is easily utilized by end-users to tackle challenges, design new programs, and create a shared mental model of an institution’s unique microenvironment. Three hospital medicine divisions across the country have actively engaged with and applied the LWE model to their unique needs. In describing these distinct innovations, we demonstrate the model’s flexibility and broad utility to frontline educational faculty, practicing hospitalists, and administrative leaders.