Background: Structured interdisciplinary bedside rounding (SIBR) has been shown to improve patient communication, patient satisfaction, and reduce clinical errors. However, there continue to be challenges in sustainable and consistent implementation due to many logistical challenges. In 2022, we implemented geographic localization for our general internal medicine inpatient services at our academic medical center. This increased the number of shared patients between nurse and physician and facilitated the ease of which to complete return visits. While we explored adapting other strategies that have been successful at other institutions to facilitate SIBR, we found significant challenges in implementing similar changes due to variability in our nursing and physicians’ practice patterns. We then proceeded with creating a custom solution to best integrate SIBR into our practice consistently.
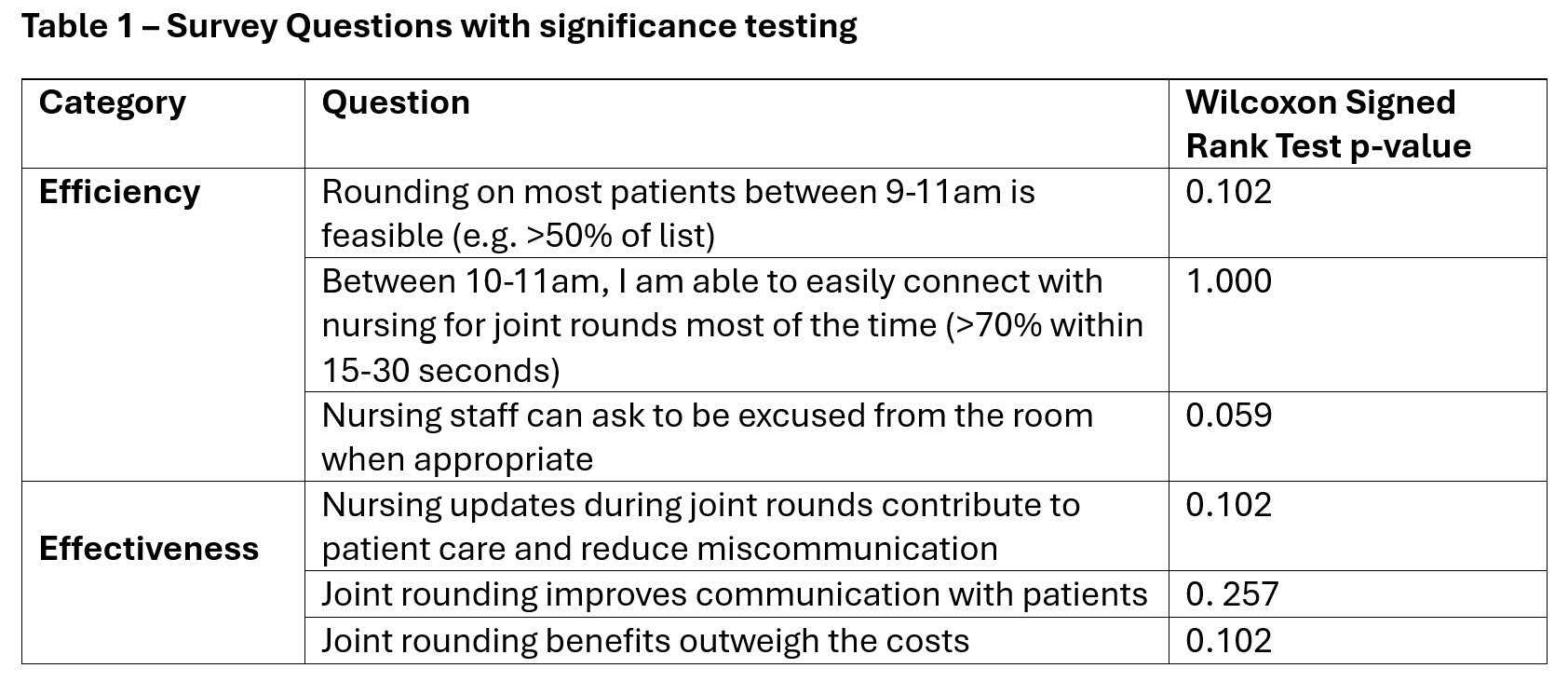
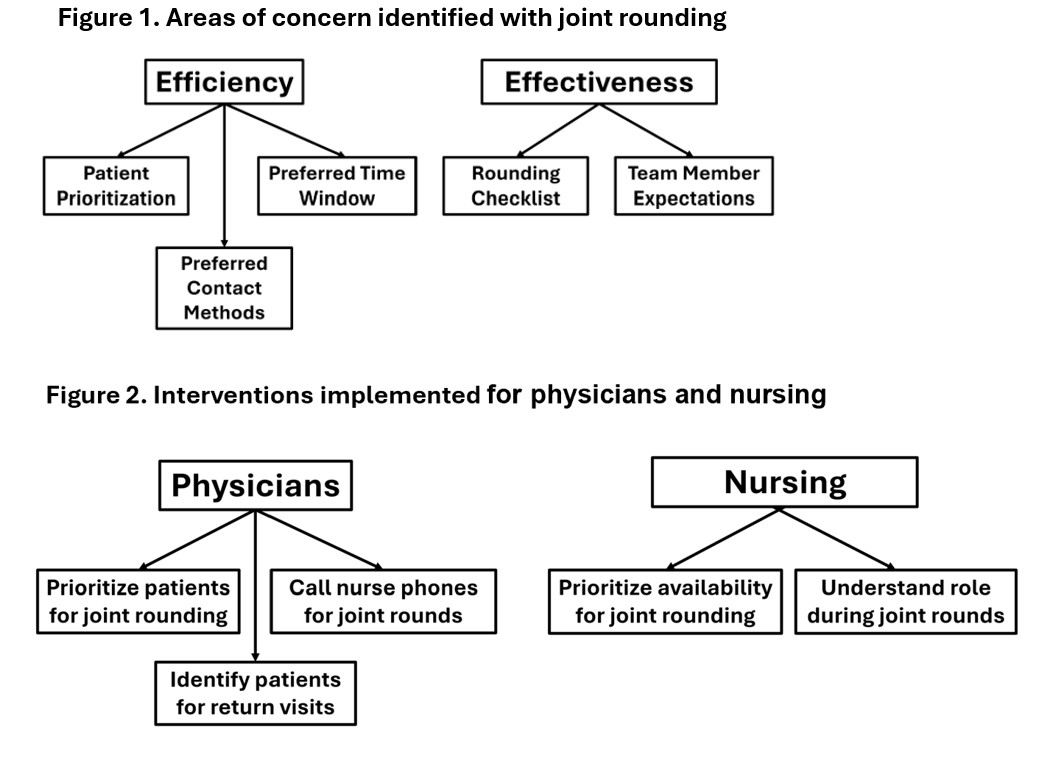
Purpose: In early 2025, we conducted surveys of our physicians and nursing staff to identify key barriers to conducting SIBR. We identified concerns regarding the ease of contacting bedside nurses, nurse availability to join at the bedside, and team member expectations. We then created recommendations to address these challenges (e.g. preferred time for joint rounds, preferred contact methods, using a rounding checklist). We then presented our recommendations at our monthly physician faculty meeting and provided pre-service email reminders for 8 weeks between May and July 2025. We also requested our nursing managers to provide education to bedside nursing staff at regular intervals. Our primary outcome metrics were HCAHPS survey scores (Likelihood to Recommend [LTR], Physician Communication). Secondary metrics included patient perception of joint rounding (via a supplemental HCAHPS survey question) and physician survey responses regarding joint rounding concerns on a Likert scale. We compared physician ratings from before and after a week on inpatient service using the Wilcoxon Signed-Rank Test to determine statistical significance.
Description: While we did not see a significant change in HCAHPS likelihood to recommend or physician communication scores during our intervention period compared to the previous year, patients who reported having had interdisciplinary bedside rounds also reported significantly better experience and communication scores. In addition, we had good physician survey return rate (48% pre-service (n=11/23), 43% post-service (n=10/23)), with survey responses revealing positive trends (p-values = 0.059 to 0.257) towards improved feasibility of performing SIBR, clarity of expectations, and effectiveness of SIBR (e.g. improved communication, error reduction, cost-benefit). There was a net neutral response towards improved ease of contacting nursing. There were no measured negative impacts from our intervention.
Conclusions: Conducting SIBR remains a high impact intervention that improves communication and teamwork between patients, nurses and physicians. Many challenges can be addressed by geographic localization of inpatient services. We next plan to integrate a Real Time Location System (RTLS) into the joint rounding workflow in the coming year to further improve coordination and data collection (e.g. joint rounding completion rates).