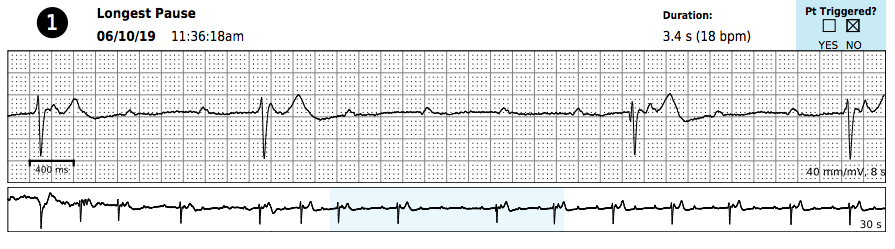
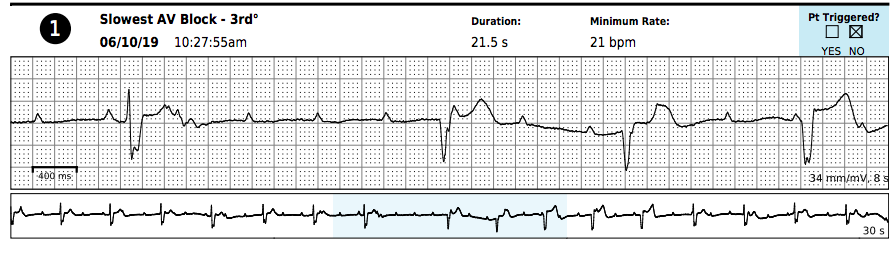
Case Presentation: A 20 year-old, asymptomatic Caucasian man presented to the Emergency Department while vacationing in New Orleans. His home physician instructed him to self-present to the nearest hospital after receiving the patient’s Holter monitor data, which noted third-degree AV block and heart rate nadir of 21. The patient was wearing a Holter monitor due to nonspecific T-wave abnormalities seen on a screening EKG, which he underwent as part of a routine exam for his pilot training.The patient reported no pre-syncopal symptoms (including during high-intensity exercise protocols in military school), no palpitations, no shortness of breath, no lightheadedness, no rash, and no fever. The patient had no past medical history and took no medications. Physical examination, including a complete skin exam, was unremarkable. He remained hemodynamically stable from admission to discharge. EKG on admission showed first-degree heart block with a PR interval of 340 ms.The initial differential diagnosis was extensive but was narrowed to Lyme disease (as the patient lived in a Lyme-endemic region of the Northeastern United States), cardiac sarcoidosis, or another rheumatologic condition leading to an infiltrative cardiomyopathy. Throughout his hospital stay, discussions were held with the patient and amongst the cardiologists and electrophysiologists regarding the implantation of a pacemaker in a patient who is so young, continually asymptomatic, and with career dreams incompatible with such a device. Without timely treatment, complete heart block can quickly be fatal. However, he had no additional episodes of complete block during his stay, continuing only to have a prolonged PR interval around 300 ms. While awaiting a PET scan, Lyme titers resulted positive, and a diagnosis of Lyme carditis was made. With the etiology being reversible, there was no indication for a temporary or permanent pacemaker. The patient was initiated on ceftriaxone until the PR was < 300 ms, after which he was transitioned to oral doxycycline.
Discussion: This was a case of completely asymptomatic Lyme carditis, even in the setting of complete heart block and sinus bradycardia to 21. Of the 45 published cases with third-degree heart block due to Lyme disease, all presented with symptoms—most commonly rash, syncope, fever, or lightheadedness (1). This Lyme diagnosis was only detected due to a routine aviation screening EKG. Untreated Lyme disease progresses to carditis in 4-10% of cases and to second- or third-degree heart block in only 1% of cases (1, 2). A handful of reports have documented sudden cardiac death. Ultimately, the patient received treatment for this reversible cause of complete heart block, avoiding pacemaker placement and allowing him to fulfill his career aspirations.
Conclusions: Life-threatening complications of Lyme disease progression, such as complete heart block, can be completely asymptomatic. Furthermore, given the potential for individuals to travel outside of Lyme-endemic regions and present in non-endemic regions, Lyme disease should be on the differential for various degrees of heart block in all states.