Background: During the COVID 19 pandemic, our organization used a novel virtual care approach, an adult hospital at home (AH@H), to address the demand for bed capacity. Our pediatric hospital faces a similar capacity issue, being over 90% bed occupancy in 2024. While some pediatric acute hospital at home (PAH@H) models are used in Europe and Australia, US health systems have not integrated this model of care into pediatric hospital medicine (1, 2). In February 2025 we launched a PAH@H program to provide acute hospital level care for patients at home to expand our pediatric bed capacity.
Purpose: Our goal is to explore implementation factors that allowed us to be the first to launch such a program in the US. We hypothesize that there were critical factors that allowed us to pilot PAH@H.
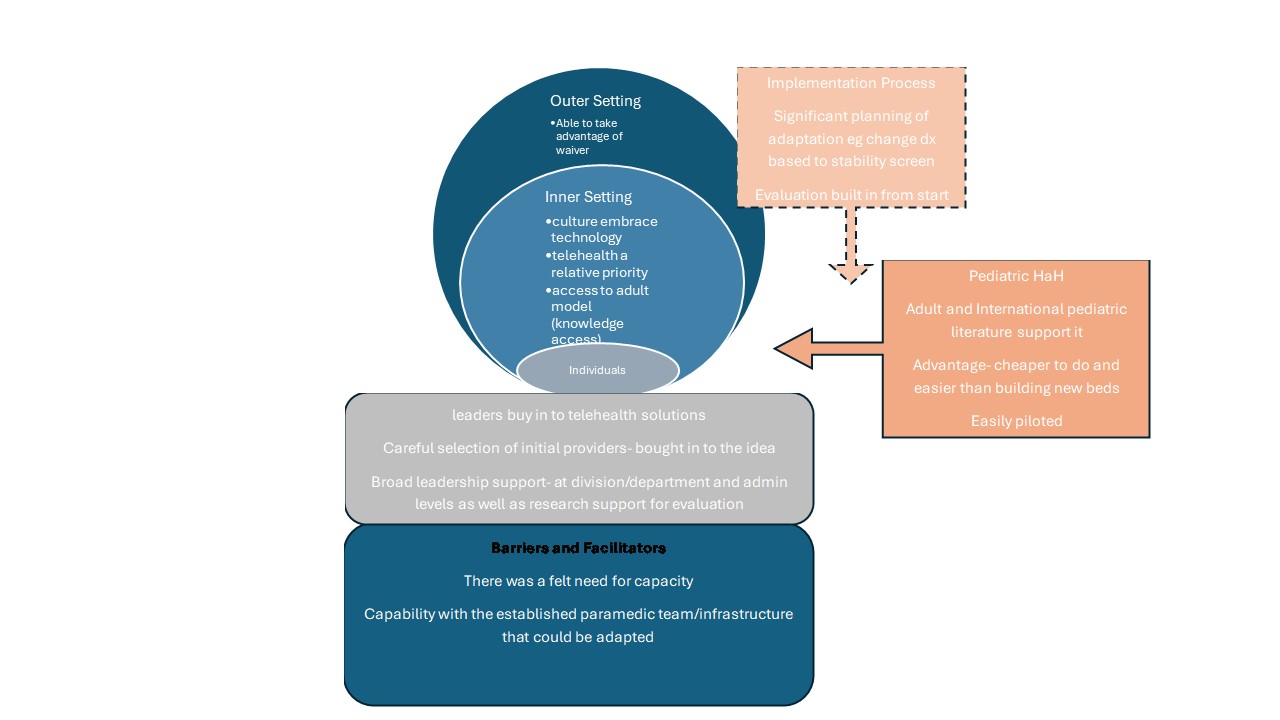
Description: We evaluated the implementation process using relevant constructs from the consolidated framework for implementation science (CFIR). Team members reviewed the constructs in the domains of Innovation, Outer Setting, Inner Setting, Individuals, and Implementation and noted key aspects applicable for our project. The key factors for launching the program were reached through consensus. The integration of AH@H in our health system as a safe, financially viable capacity expander for the adult population provided a model to adapt to pediatrics with internal experts and a team that could be scaled. Our health system management is an early adopter of virtual health, identifying it as an expanding area for clinical excellence. Our pediatric bed shortage provided a need for a creative solution. Respected leaders drove the implementation by using this situation to build the model while meeting needs like clinical triaging and research capacity development. These factors allowed the team to secure funding to develop a pilot program using the CMS Hospital at Home waiver regulations. See Figure 1 for applicable CFIR constructs.
Conclusions: Launching a successful PAHaH program requires a felt need such as bed capacity, system support for the model and its financing, and scalability. The long planning and implementation cycle for PAH@H revealed that careful thought on integration into existing hospital systems of finance, research, clinical protocols, process flow mapping, and proper selection of care team participants are required for a successful program start. The preexisting CMS Hospital at Home Waiver reduced the barriers to entry for our program. Future work is needed to ensure other PAH@H programs can launch to meet the needs of their specific patient groups in a timely and efficient manner.