
Background:
At the time of a major surgery, patients requiring chronic oral anticoagulation therapy must have had this treatment either stopped and restarted or “bridged,” substituting heparin or low‐molecular‐weight heparin (LWMH) except during and shortly after the procedure. It is not clear how these patients are currently being managed and how frequently bleeding and thrombotic outcomes occur.
Methods:
This was a prospective 9‐hospital observational study. Periprocedure bridging anticoagulation was classified a priori as: (a) none, (b) prophylactic dose heparin/LMWH, or (c) full‐dose heparin/LMWH. Outcomes included method of management and 30‐day incidence of thromboembolic and bleeding events.
Results:
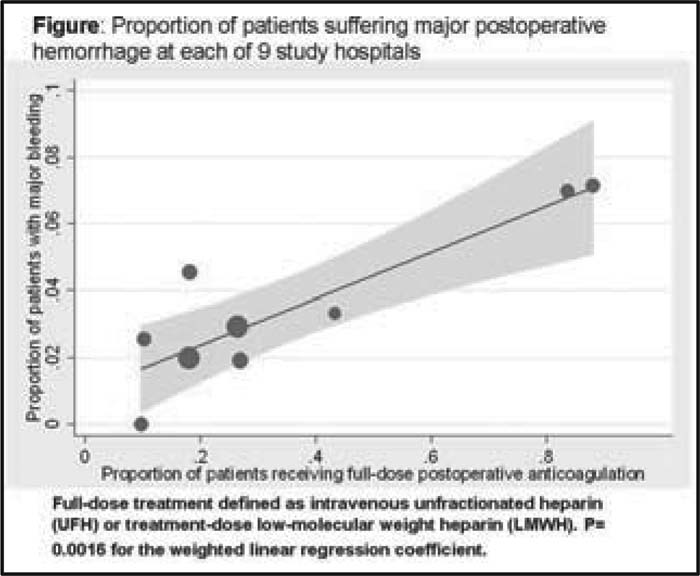
Four hundred and ninety‐two of 497 consecutive patients (99%) completed the study. The postprocedure dosing of heparin/LMWH was: none in 54%, prophylactic in 14%, and full dose (therapeutic dose) in 33%. Two hospitals treated more than 80% of their patients with full‐dose heparin, whereas the remaining 7 hospitals used full‐dose heparin in an average of 22% of cases (P < .0001 for overall heterogeneity). This heterogeneity in practice pattern was not accounted for by differences in patient characteristics or the types of surgery (adjusted P < .0001). There were 4 thromboembolic events (0.8%; 95% CI: 0.3‐2.1) and 16 major bleeding events (3.2%; 95% CI: 2.0‐5.2). After adjustment for surgical and patient‐specific bleeding risk, use of full‐dose hepa‐rin/LMWH postprocedure remained associated with significantly higher likelihood of major bleeding: odds ratio 4.4 (95% CI: 1.5‐14.7).
Conclusions:
Management of anticoagulation after an invasive procedure varies widely. The risk of major bleeding was substantial and significantly associated with use of therapeutic doses of heparin/LWMH. Randomized trials are needed to compare the risks and benefits of using different heparin/LMWH bridging strategies perioperatively.
Author Disclosure:
R. H. White, Astra‐Zeneca International, grant funding; A. K. Jaffer, Astra‐Zeneca International, consulting.