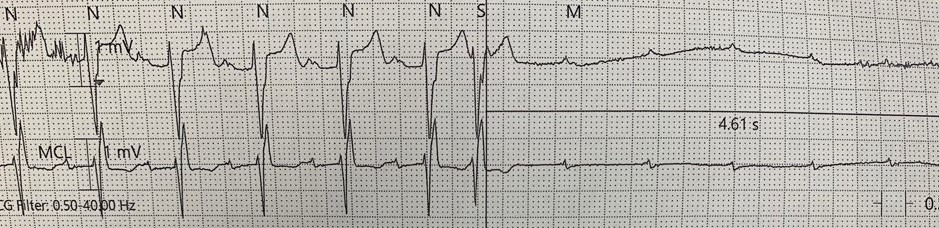
Case Presentation: A 68-year-old woman with a history of remote coronary artery bypass surgery and aortic valve replacement presented with multiple syncopal episodes. The patient was in her usual state of health until three months prior to presentation when she experienced an episode of dizziness quickly followed by loss of consciousness. Multiple similar episodes of syncope occurred over next three months, until the day of presentation when the patient experienced a syncopal episode while ambulating in public, prompting a bystander to call emergency medical services. The patient was brought to the emergency department where initial electrocardiogram was notable for sinus rhythm with a right bundle branch block, left anterior fascicular block, and first-degree AV block. After admission, telemetry was notable for recurrent episodes of third-degree AV block, always preceded by sinus pauses and typically following atrial premature contractions, ultimately requiring a transvenous pacemaker. The patient underwent an uncomplicated dual chamber pacemaker placement prior to discharge on hospital day six.
Discussion: The cardiac action potential is divided into four phases. During phase 4, the resting membrane potential, spontaneous depolarizes occurs in nodal tissue leading to automatic activity. While spontaneous depolarization is typically suppressed in His/Purkinje cells, in patients with advanced conduction disease non-nodal conduction tissue may gain this property. In such cases during long cycle lengths such as following premature beats or sinus pauses, conduction tissue may inappropriately depolarize leaving the membrane refractory to further impulses and resulting in sudden atrioventricular block. This pause-dependent or phase four block is a relatively rare cause of paroxysmal heart block, reported in approximately 12% of cases. As these cases are typically associated with advanced conduction disease, escape rhythms are unreliable, making these patients high risk for syncope. Phase 4 block can be precipitated by atrial or ventricular premature beats, sinus bradycardia, or following the termination of a supraventricular tachycardia. Pacemaker implantation is the mainstay of treatment in these patients and as such it is important to distinguish this entity from benign vagally mediated pauses which typically would not require permanent pacemakers. While both are associated with preceding bradycardia or pauses, vagally mediated pauses occur more gradually and are associated with sinus slowing during periods of block. In pause-dependent AV block however, there will be a compensatory increase in the underlying sinus rate.
Conclusions: Paroxysmal atrioventricular (AV) block is defined as the sudden block of atrial impulses in the setting of otherwise one-to-one AV conduction and typically occurs in patients with underlying conduction disease. Due to the unique characteristics of diseased conduction tissue, particularly in phase four of the cardiac action potential, these episodes are often preceded by bradycardia or sinus pauses. Escape rhythms in this condition are unreliable, often leading to recurrent episodes of syncope in impacted patients. Phase four AV block is a rare but important cause of paroxysmal AV block. Early recognition and pacemaker implantation are vital to preventing morbidity in effected patients.