Background: Point of care ultrasound (POCUS) has become an integral part of the physical examination and a valuable diagnostic tool. POCUS is unique among medical technologies in that it requires physical co-location of the provider and patient. Previous studies have shown the value of shared decision-making between patients and providers requiring a mutual understanding of both the diagnostic process and the patient’s diagnoses. The effect on shared understanding of adding POCUS to the traditional examination is unknown, yet this is an often described benefit of POCUS. The primary aim of the study was to determine if the use of POCUS improves shared understanding between providers and patients about diagnoses.
Methods: This is a prospective, controlled trial involving a convenience sample of hospitalized adults under the care of a hospitalist. Providers were assigned to either the control arm or the study arm in a 1:1 fashion. The providers in the control arm performed usual care without POCUS, while providers in the study arm had the option to add POCUS. Data was collected on two random, blinded days for each provider during each study week, avoiding the first and last days of the week. Subjects were approached for enrollment in the study after electronic health record screening. After consent was obtained, a survey was administered to the subjects with questions on patient understanding of symptoms, diagnosis, and main contributors to their health problem. Later in the day, study staff contacted the attending physician to complete the corresponding provider survey for each subject enrolled that day. At the end of the study, two independent physicians rated the degree of shared understanding between patient and provider surveys with respect to the patient symptoms at presentation, their diagnosis and key contributors to their diagnosis. The ratings of the two independent physicians were averaged across each domain and means were calculated. Means were compared between the two study arms using exact Wilcoxon 2-sample tests.
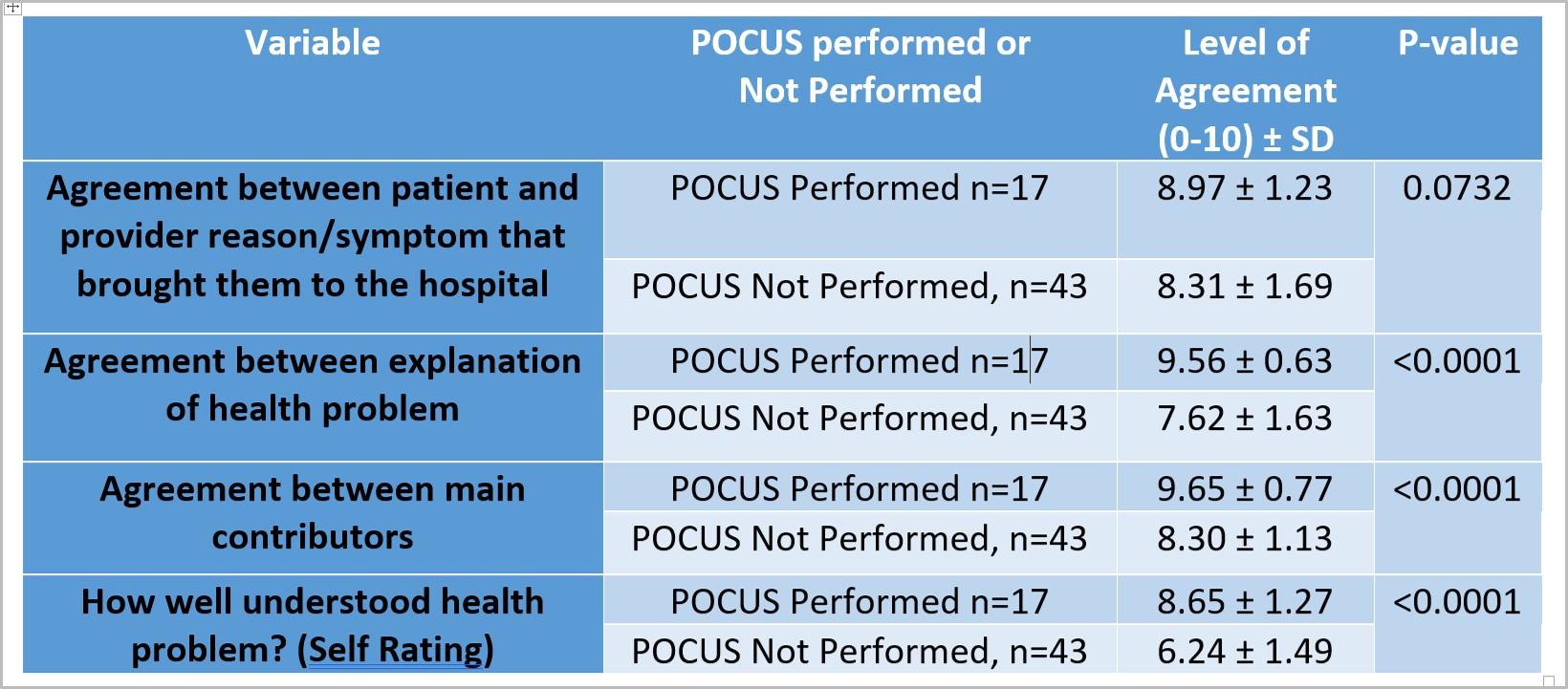
Results: Of the 64 patients enrolled in the study. 60 had complete data and were included in the analysis. There were 10 total providers, each arm having 5 providers with equal experience levels. There was increased shared understanding between providers and patients with respect to their symptoms, (POCUS 8.97 ± 1.23, non-POCUS 8.31 ± 1.69, p=0.073), diagnosis (POCUS 9.56 ± 0.63, non-POCUS 7.62 ± 1.63, p <0.005), and main contributors (POCUS 9.65 ± 0.77, non-POCUS 8.30 ± 1.13, p <0.005) in the POCUS arm compared to the non-POCUS arm. In keeping with the improved shared understanding, patients also had increased self-rating of their understanding of their health problem in the POCUS arm compared to the non-POCUS (8.65 ± 1.27 versus 6.24 ± 1.49, p<0.005). Both providers and patients thought POCUS was valuable when performed (mean rating for both groups was 3.76/4 + 0.44).
Conclusions: Patients in the POCUS arm had a significantly higher understanding of their health problem as well as the information their provider used to arrive at that diagnosis. These findings suggest that using POCUS improves patients’ understanding of the diagnostic process and aids in communication with patients. There are multiple previous studies that show that POCUS improves diagnostic accuracy and efficiency. Combined with previous data, our findings suggest that POCUS may be a tool uniquely poised to improve not only the outcomes of the diagnostic process but also enhance patients’ understanding of and engagement in that process.
.jpg)