Background: Patients with complex medical problems are at high risk of readmission when transitioning from the hospital to home, especially when they reside in rural areas (as is the case within our VA Health Care System (HCS)). Innovative solutions are needed to improve access to post hospitalization follow up within our facility. We hypothesized that virtual technology will improve timely post discharge follow up by overcoming limitations such as the need for transportation and bad weather. Here, we report our experience in implementing a virtual transition of care clinic (TOCC).
Purpose: To identify barriers to implementing virtual TOCC.
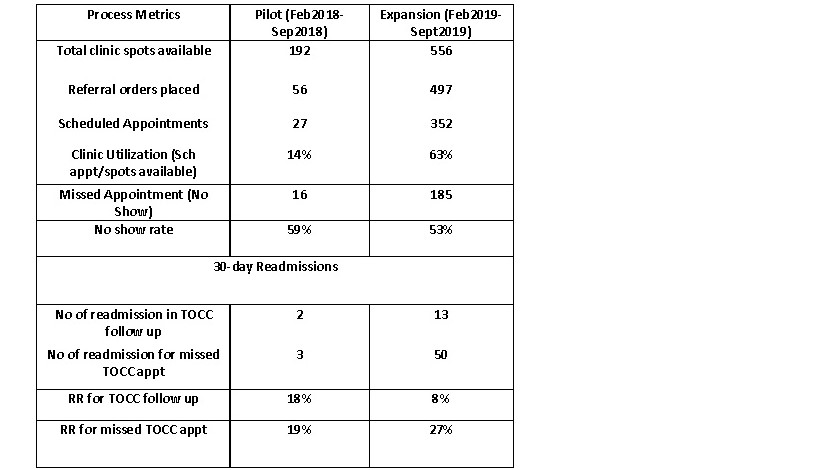
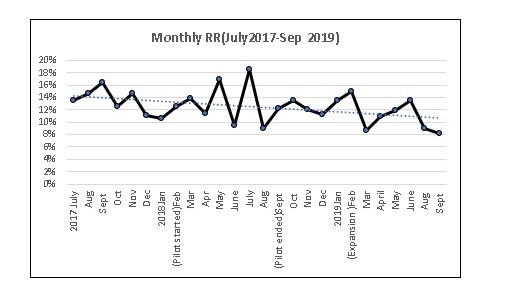
Description: The virtual TOCC is designed to address post discharge needs including medication reconciliation and changes in health status after discharge. The patient visits are supported by a HIPAA-compliant video interface. The tablet is introduced to the patient at the bedside prior to discharge via the discharge coordinators and then mailed to the patient within 48 hours of referral. We first piloted the clinic for 6 months by offering 2 clinics per week. The pilot focused on congestive heart failure (CHF) patients as they had the highest readmission rate (RR). This was followed by an expansion phase.We met monthly and the Plan-Do-Study-Act (PDSA) cycle was applied to implement solutions. Barriers identified during the pilot phase included limited clinic days, patient reluctance to use a tablet device, delays in tablet delivery, and lack of an assigned scheduler. Solutions included: creating daily clinics, offering face-to-face visits, active IT support, and dedicated scheduler support. These solutions allowed us to expand the clinic to all high-risk patients requiring close post-discharge follow up. During the more recent PDSA cycles new barriers were identified including lack of TOCC awareness among the new resident inpatient teams, unexpected nationwide tablet shortage, hesitation to refer patients due to the national tablet shortage, and limited case-manager support. The following solutions were implemented: TOCC is introduced to the inpatient resident teams during site onboarding followed by weekly reinforcement, the scheduler provides the patients alternate methods of follow up (face to face or primary care) in cases of delayed tablet delivery, discharge planner and IT education regarding the alternative follow up options. Further support is being sought for a full-time case manager and we are exploring the feasibility of patient visits utilizing video stations at the community-based VA clinics.The process metrics measured are shown in the Table below. We noted increased utilization of TOCC over time.The RR between March-September 2019 was significantly lower for the patients seen in TOCC (8%) versus those that were not seen in TOCC (27%). Reasons for no show included patients forgetting the appointment, seen by PCP due to double scheduling, inability to reach patients via the tablet device, and delays in tablet delivery. Based on the facility monthly RR data (shown in the Figure), there was a trend towards reduction in RR during the TOCC expansion phase (2019).
Conclusions: We report that the implementation of virtual post discharge follow up for patients at high risk of readmission is feasible and appealing to many patients in the VAHCS. Further research is needed to evaluate patient and system factors that may impede or facilitate participation in virtual follow up and to compare the efficacy of virtual versus face to face visits in improving outcomes.