Background: Adverse events (AEs) after discharge occur in 19–28% of hospitalized patients.(1) Understanding whether patient-reported and clinical factors from the electronic health record (EHR) can predict post-discharge AEs is increasingly important given the growing population of hospitalized adults with multiple chronic conditions (MCC) being discharged home. This AHRQ-funded study aimed to develop an interoperable prediction model of post-discharge AEs using standardized patient-reported outcomes (PRO) and structured EHR data, including widely available risk prediction scores.
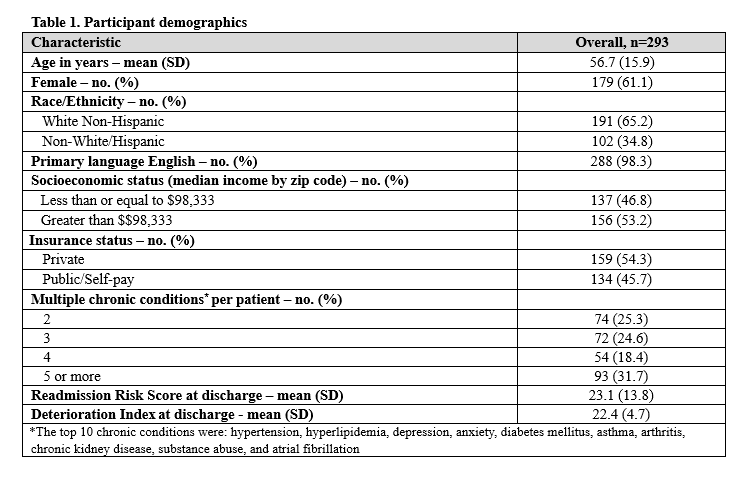
Methods: This IRB-approved retrospective analysis included 293 hospitalized patients with two or more MCCs discharged from general medicine services between February 2022 and August 2023 at an academic medical center in Boston, MA using a single EHR (Epic Systems, Inc.). All patients completed the 10-item global health PROMIS questionnaire at discharge. A validated chart review and 2-clinician adjudication process was used to determine whether one or more AEs occurred within 14- or 30 days post-discharge.(2) Twelve candidate predictors were identified based on literature and expert opinion, including demographics, medication changes, pending studies, Epic’s readmission risk, deterioration index, and global health PROs. All variables were retrieved from the EHR at discharge or computed from the PROMIS questionnaire (physical or mental health score). We conducted multivariable logistic regression to model 14-day or 30-day AEs and the c-statistic was calculated.
Results: The characteristics of 293 patients are shown in Table 1: 66 (22.5%) and 90 (30.7%) experienced an AE within 14-days and 30-days post-discharge, respectively. Adjusted analyses (Table 2) showed that a moderately elevated deterioration index (>20) (OR 2.65 [1.21, 5.81], p= 0.01) and a low mean arterial pressure (OR 1.90 [1.00, 3.62], p = 0.05) were independently associated with 14-day post-discharge AEs. Female sex (OR 1.91 [0.97, 3.75], p=0.06) and non-White race / ethnicity (OR 1.87 [0.95, 3.69], p=0.07) approached but were not significant. A low mean arterial pressure (OR 1.90 [1.07, 3.36], p = 0.03) was independently associated with 30-day post-discharge AEs. Global-10 derived physical and mental health scores were not associated with 14-day or 30-day AEs. The c-statistics were 0.69 and 0.65 for 14-day and 30-day post-discharge AEs, respectively.
Conclusions: In this cohort of hospitalized patients with MCCs, multivariable models demonstrated modest discrimination for predicting post-discharge AE within 14-days of hospitalization¸ largely attributed to indicators of clinical deterioration or hemodynamic instability. Neither the readmission risk score nor PRO measures were associated with AEs. Integrating variables related to deterioration into discharge planning processes may improve detection of patients at high risk for AEs. Future studies should validate these findings for different populations and settings.