Background: Mental illness is common among hospitalized patients and is associated with increased length of stay, higher costs, and worse clinical outcomes. Inpatient psychiatry consultations have traditionally held a reactive model, in which primary teams obtain consultation for patients that have developed active psychiatric symptoms. The reactive model has frequently led to missed opportunities to address mental health issues, increased length of stay due to late recognition of active psychiatric problems, and suboptimal coordination of post-discharge mental health services. Some hospital programs have adopted a proactive approach to psychiatry consultation to address co-morbid psychiatric conditions among hospitalized patients, though the data on program outcomes and cost savings are still emerging.
Purpose: We describe a program in which a psychiatric consultation service was embedded in Medicine Units primarily staffed by hospitalists. The goals of the program were to identify and intervene on patients with psychiatric needs before problems arise. Outcome measures included length of stay (LOS) and cost savings.
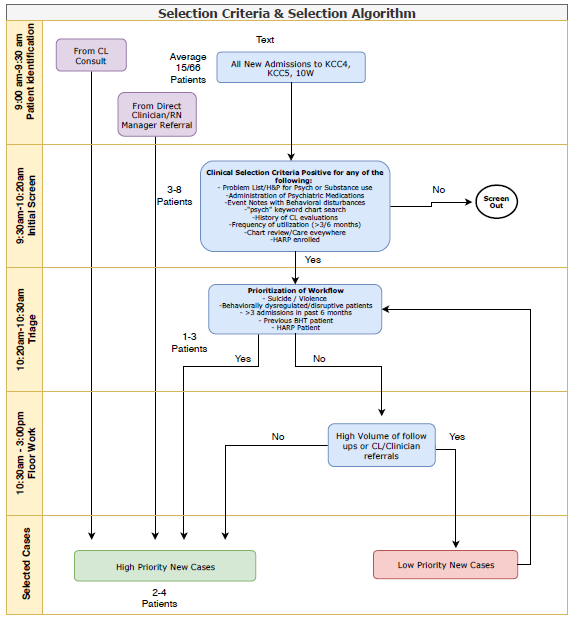
Description: This clinical program was conducted at a large urban academic hospital. The program enacted a multi-disciplinary team, referred to as the Behavioral Health Intervention Team (BHIT), composed of social worker, psychiatrist physician, and nurse practitioner. This team was linked to three inpatient Medicine units staffed by hospitalists. The clinical goal of the BHIT was to address behavioral barriers to medical care, avoid psychiatric crisis, and lend support to the clinical floor staff for patients with psychiatric co-morbidities admitted to these units. When active psychiatric symptoms emerged, the BHIT also provided guidance for treatment recommendation and crisis management. Patients were screened in by BHIT and by unit nurses and hospitalist physicians (figure 1). In 2018, the BHIT program screened in 365 unique consultations as compared to 191 on the traditional service the previous year. This represented a 91% increase in cases seen over the course of a year. Among patients seen by BHIT, the average LOS was 10.5 days compared to 18.5 days for those seen under the traditional model. For inlier patients with LOS < 31 days, this pattern held with 350 patients seen by BHIT with average LOS 8.4 days, compared to 164 patients seen in the traditional model with average LOS at 11.5 days (p=0.004). This reduction in LOS represented potential savings of $1,260,000 across a twelve-month period.Clinician feedback on the program was largely positive, with survey comments indicating reduction in clinician anxiety, unit staff feeling support with de-escalating “messy” situations, staff valuing integrated multi-disciplinary approach, and staff appreciating consistent BHIT members who were embedded within the units and easy to contact.
Conclusions: Adoption of a multi-disciplinary team dedicated to addressing psychiatric co-morbidities in hospitalized patients led to decreased length of stay and increased cost-savings. When embedded into Medicine units, the proactive BHIT team was able to see many more patients than a traditional consultation model. Subjective program appraisal by floor staff was universally positive.