Background: Sepsis, a dysregulated host immune response to infection leading to life-threatening organ dysfunction[1], is a common, fast-moving condition, and the leading cause of in-hospital death. Most cases develop in the community and present to Emergency Departments (ED)[2], where urgent action is required to prevent resultant morbidity and mortality[3]. However, the presentation of sepsis is nonspecific, making the diagnosis difficult, especially in early stages when intervention is most efficacious. One readily available stratification method that has been gaining traction is ICU level of care (ICU LOC). In this study, we assessed the risk-stratification value of ICU LOC compared to a cellular host-response test (HR) in a population of suspected infection patients.
Methods: A semi-quantitative in-vitro HR test uses deformability cytometry to assess leukocyte biophysical properties from whole blood in < 10 min. The test generates an Index (0.1 - 10.0), stratified into 3 interpretation bands (Band 1, Band 2, Band 3) of increasing sepsis likelihood[4].Adult patients presenting to the ED with signs or suspicion of infection were prospectively enrolled at multiple US sites (02/2016–10/2021). EDTA-anticoagulated blood was assayed within 5 hours from draw using the test, and patients were followed by retrospective chart review. Infection and sepsis status were determined via retrospective physician adjudication per Sepsis-3 criteria. Necessity for ICU care (ICU -/+) was determined through objective cardiovascular (MAP < 60 or SOFA-CV ≥2), respiratory (PF ratio < 200), or renal ([Creatinine > 5 and (HCO3- < 12 or K+ > 6)] or BUN > 120) criteria within 3-days of presentation. Missing data was not imputed.
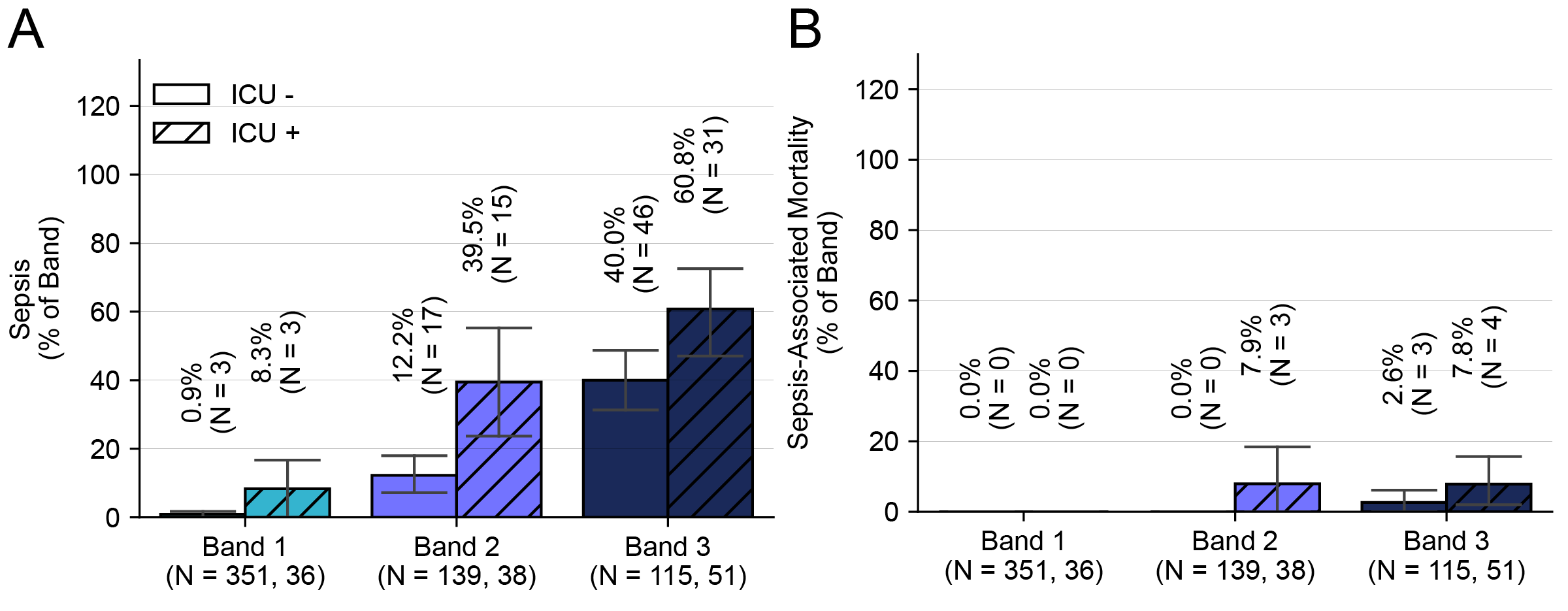
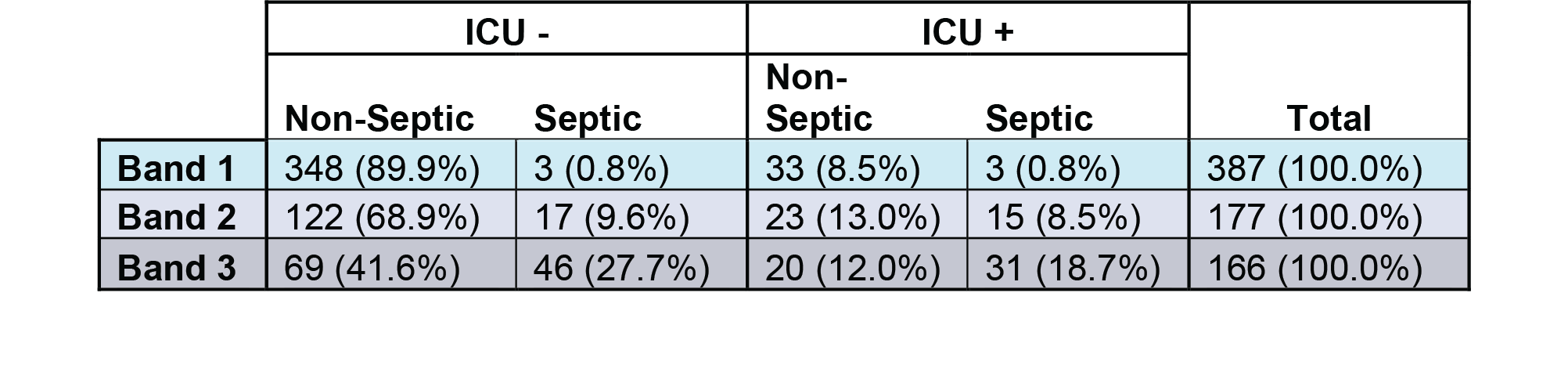
Results: We analyzed a cohort of 730 patients (sepsis prevalence 19.2%) and found 605 patients (82.9% of total) did not meet necessity for ICU level of care (ICU-) and 125 (17.1%) met at least one criteria (ICU+, Table 1). The ICU- cohort consisted of 351 (58.0%) Band 1, 181 (23.0%) Band 2, and 115 (19.0%) Band 3 patients, while the ICU+ cohort consisted of 36(28.8%) Band 1, 38 (30.4%) Band 2, and 51 (40.8%) Band 3. Across all interpretation bands, the most common criteria for ICU+ patients was respiratory (49.0%), followed by cardiovascular (45.3%) and renal (5.7%), with 19.5% of patients meeting multiple criteria. The majority of patients retrospectively adjudicated septic were in the ICU- group (N=66, 57.4%). Furthermore, 30% of sepsis-associated mortalities were observed in this ICU- group (Table 1). Regardless of ICU care necessity, the HR test achieved appropriate diagnostic performance and risk stratification, with increasing rates of sepsis-3, and sepsis-associated mortality across increasing interpretation bands (Fig 1 A,B). Notably, there were no Band 1 patients with sepsis-associated mortality in either of the ICU- or ICU+ cohorts (Fig 1 B). Finally, the diagnostic performance of the HR test for risk of sepsis was observed to be similar irrespective of the need for ICU level of care (ICU- : Sensitivity – 95.5% [87.1-99.1%], Specificity: 88.5% [77.5-94.6%]; ICU+: Sensitivity – 91.8% [80.4-97.7%], Specificity: 73.7% [58.9-85.1%]).
Conclusions: The results of this study suggest both that ICU level of care is an inappropriate metric for the identification of sepsis and it’s severity and that a host response test for early sepsis detection and risk stratification in the ED may provide a more specific solution.