Background: Recent data suggest that there are mortality benefits from preoperative statin therapy in patients at high risk for atherosclerotic cardiovascular disease (ASCVD). Current guidelines recommend moderate or high intensity statin for all patients with established ASCVD or 10-year risk of > 7.5%. In our preoperative evaluation clinic which is staffed by hospitalists, there were many patients who were observed to either not be on statin or were on lower doses than recommended. We estimated 20% of our patients would not be on appropriate statin therapy and a lower limit of the 95% confidence interval (CI) of 15% would be enough to change our preoperative screening process.
Methods: In this retrospective chart review, we examined 200 patient patients presenting to a perioperative optimization clinic at a single, urban, tertiary-care center. We collected demographic and clinical information to calculate a 10-year ASCVD risk score (using the 2013 ACC/AHA pooled cohort equation) as well as statin use. The proportion of any patients on no or suboptimal dose statin with 95% CI were calculated.
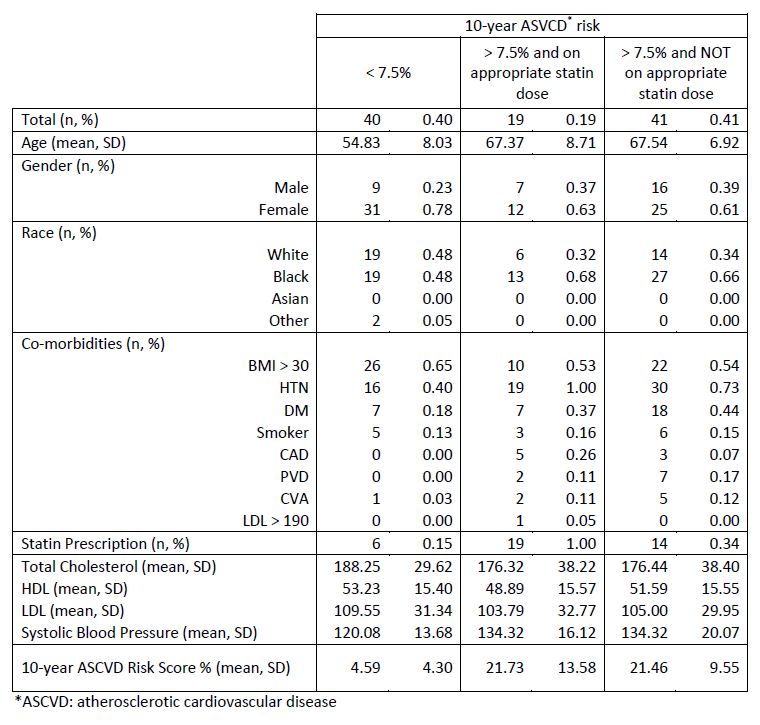
Results: 100 (50%) of all patients had information available to calculate a 10-year risk score. Of the 100 patients, 40 had a low risk score of < 7.5% and 60 had a risk score of > 7.5%. Of patients with high risk score 19/60 (32%) were on appropriate dose of statin, 14/60 (23%) were on suboptimal dose and 27/60 (45%) were not taking a statin. 41% (95% CI 32-51%) of patients with risk score > 7.5% were either on inappropriately low or no statin therapy.
Conclusions: Only half of patients seen in our preoperative clinic were age 40-79 (age in which the risk equation is applicable to) and/or had cholesterol data available to calculate of a 10-year cardiovascular risk. When able to calculate 10-year cardiovascular risk, at least a third (lower limit of 95% CI 32%) were not on appropriate statin therapy and we plan to initiate cardiovascular screening and statin initiation into our preoperative clinic workflow.