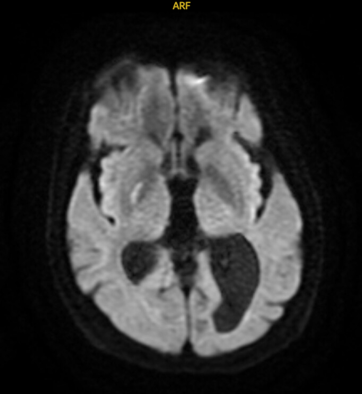
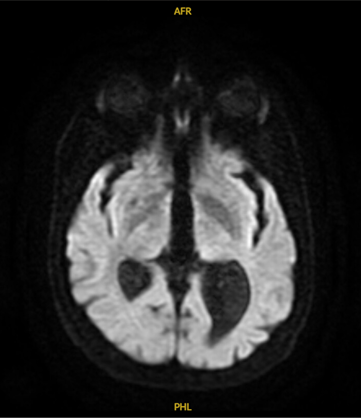
Case Presentation: A 67-year-old woman with hypothyroidism, managed on levothyroxine, presented as a stroke alert due to sudden onset of left facial droop, slurred speech, and irregular, jerking movements of the left limbs. These symptoms initially began during a prior hospitalization. She exhibited partial voluntary control over the movements, raising suspicion for a possible functional or psychiatric component. The involuntary movements worsened with emotional stress, improved with relaxation, and could be partially suppressed. There were no additional neurological or systemic symptoms, no history of substance use; recent psychosocial stressors included a recent marriage, caregiving responsibilities, and relocation.During her second admission, her facial droop and aphasia persisted. MRI confirmed an acute ischemic lacunar infarct in the basal ganglia. Echocardiogram revealed a patent foramen ovale. Neurology attributed the left-sided involuntary movements to post-stroke vascular hemiballismus. The patient was prescribed benztropine 1 mg three times daily and advised to follow up as an outpatient with a movement disorder specialist.
Discussion: This case presents a unique scenario where the typically involuntary condition of vascular hemiballismus could be temporarily controlled through distraction and self-relaxation techniques. It suggests that physiological changes such as excitation or stress may influence this disease process.The primary neurotransmitter imbalance in hemiballismus involves increased excitatory and decreased inhibitory signals. Normally, the subthalamic nucleus (STN) receives inhibitory input from the globus pallidus, often disrupted in hemiballismus. This disruption leads to STN overactivity and increased excitation in the thalamus and motor cortex. Vascular events can impair cerebral blood flow to neurons in the globus pallidus, reducing transmission of gamma-aminobutyric acid (GABA), the primary STN inhibitor. This case suggests a possible transient restoration of GABAergic function linked to decreased psychological excitation.The patient’s GABAergic neurons in the globus pallidus may have sustained only mild ischemic damage during the stroke, allowing occasional inhibitory control of the STN. MRI during the patient’s second admission showed restricted diffusion in the basal ganglia, consistent with vascular hemiballismus. Fluctuations in psychological state may have influenced blood flow to GABAergic neurons.Psychological excitation activates the sympathetic nervous system, releasing vasoactive compounds like norepinephrine, which acts on adrenergic receptors in cerebral vessels, causing vasoconstriction. Conversely, relaxation activates the parasympathetic system, promoting release of vasodilators like nitric oxide. These shifts in vasoactive compounds or neurotransmitters may redirect blood flow or alter neuronal activity, enabling temporary STN inhibition and symptom control in this case.
Conclusions: This case challenges the notion of hemiballismus as purely involuntary by showing mixed vascular and psychiatric components. Clinicians should consider psychogenic overlays in atypical cases. Psychological state may alter cerebral blood flow and neurotransmitter dynamics, offering potential adjunctive therapeutic targets. Future research should explore neurovascular sensitivity to emotional states and integrative treatments for movement disorders.