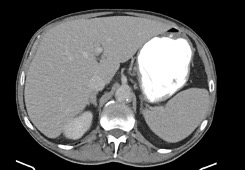
Case Presentation: A 65 year old male with hypertension, type II diabetes, heart failure with recovered ejection fraction and emphysema with 30 pack year smoking history started to experience 15 pound weight loss and anemia 18 months ago. Initial presentation to PCP revealed elevated ALP 292U/L and Hemoglobin 12.6g/dL. Cancer screening with CT chest showed multiple nodules measuring up to 5 mm and mild central bronchial wall thickening. Anemia workup with colonoscopy revealed multiple large sessile and pedunculated polyps with histopathology of tubular adenomas. Within 2 weeks progressive abdominal discomfort, constipation and increased generalized bone pain prompted him to present to the hospital. Admission bloodwork revealed elevated calcium 15.4mg/dl, creatinine 3.44mg/dl, ALP 278U/L, GGTP 203 U/L while AST, ALT, total and direct bilirubin, albumin, and platelets were normal. Subsequent testing revealed low PTH 11 pg/ml, normal 25-hydroxy Vitamin D 31.1ng/ml, 1,25-hydroxy vitamin D 73.2 pg/ml and elevated PTH-rP 4.9. Serum IF revealed low concentration of IgG kappa monoclonal protein with Kappa/Lambda light chain ratio elevated to 1.68 and urine IF negative for free light chains. ACE was negative. CT abdomen and pelvis showed hepatomegaly without hepatic lesions (Fig 1).The patient’s hypercalcemia responded to IV fluids, calcitonin and pamidronate. Follow up liver biopsy revealed non necrotizing granulomatous hepatitis. Other causes of granulomatous hepatitis were ruled out by negative ANA, negative mitochondrial antibody and non-reactive HIV 1 and 2 AG/AB. Diagnosis of hepatic sarcoidosis was made. Patient was started on prednisone with subsequent decrease in ALP level.
Discussion: The presentation of isolated liver sarcoidosis can vary, from asymptomatic to symptomatic nausea, vomiting, signs of hepatosplenomegaly, cirrhosis and liver failure. Unrecognised and untreated hepatic sarcoidosis can lead to severe complications and significant morbidity. Long standing complications include portal hypertension, liver cirrhosis and liver transplant, with the latter leading to disease recurrence in the graft. Given the aforementioned deleterious sequelae, early clinical awareness of sarcoidosis presenting as isolated hepatic sarcoidosis is important. Moreover, while the majority of sarcoidosis-related hypercalcemia is non-PTH mediated there are exceptions with increasing case reports of PTHrP mediated hypercalcemia, as seen in our patient. PTHrP is commonly thought to be a paraneoplastic phenomenon associated with hypercalcemia of malignancy. Its association with sarcoidosis is underrecognized and warrants further investigation.
Conclusions: Sarcoidosis a complex disease with significant morbidity can be fatal if untreated. The unusual extrapulmonary presentations highlight the need of a high degree of suspicion especially when encountering unexplained hepatomegaly. Furthermore, presence of PTHrP mediated hypercalcemia indicates a potential underrecognized association with sarcoidosis suggesting a need for further exploration of its role within the disease’s spectrum.