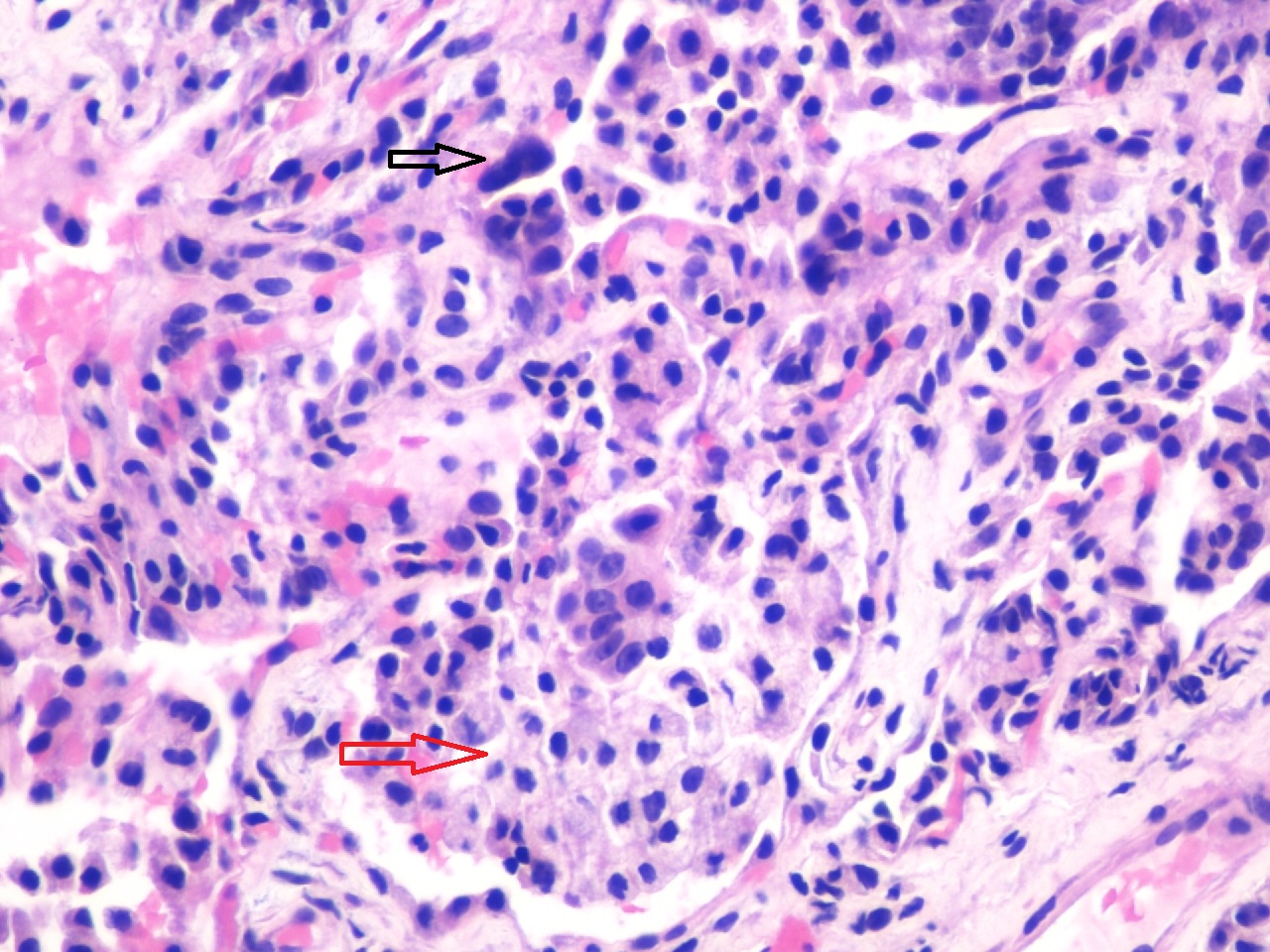
Case Presentation: A 33-year-old woman presented to the hospital following seven days of persistent fever and non-productive cough despite a course of azithromycin prescribed by her primary care physician. She denied shortness of breath, chest pain, palpitations or lower extremity swelling. She reported no sick contacts or travel in the last six months. She endorsed use of vaping tetrahydrocannabinol (THC) oil for three years but denied use of tobacco or other illicit drugs. On presentation, she was afebrile but her SpO2 was 85% on room air. Lung exam demonstrated bibasilar crackles. Laboratory results were notable for a WBC of 6.5k/uL, thrombocytosis to 480k/uL, elevated ESR (111mm/hr) and CRP (26 mg/dL). Infectious workup was negative, including HIV. Rheumatologic workup was only revealing for elevated ANA (1:320) and low C4 (10 mg/dL). CTA was negative for pulmonary embolism but demonstrated diffuse bilateral groundglass opacities. The patient was initially started on intravenous antibiotics for community-acquired pneumonia, but suspicion was raised for e-cigarette or vaping product use-associated lung injury (EVALI). A bronchoscopy and transbronchial biopsy were performed and cytology on bronchoalveolar lavage fluid was remarkable for alveolar macrophages and chronic inflammatory cells with no organisms detected. Microscopy of alveolar parenchyma showed increased intra-alveolar histiocytes with intracellular lipid and focal reactive type II pneumocytes (Figure 1). This biopsy was consistent with lipoid pneumonia secondary to EVALI. She was started on methylprednisolone and transitioned to a prednisone taper. Despite high oxygen requirements, the patient remained largely asymptomatic throughout the hospital course and was discharged on a prolonged prednisone taper. She was seen in the pulmonology clinic two weeks after discharge and reported feeling well. A follow up CT chest obtained two months after discharge showed resolution of ground glass opacities.
Discussion: Lipoid pneumonia secondary to EVALI is a diagnosis recently in the spotlight as of fall 2019. Prior to EVALI, exogenous lipoid pneumonia was a relatively uncommon diagnosis in healthy adults and was generally caused by aspiration or inhalation of fatty substances such as oil-based laxatives or oily nasal drops. This patient’s presentation was similar to other EVALI patients whose presentations have included respiratory symptoms and constitutional symptoms 95% and 85% of the time, respectively. Bronchoalveolar lavage revealed lipid-laden macrophages, a finding consistent with EVALI as pulmonary macrophages cannot metabolize oil and it is simply released back into the alveoli upon cell death. Although the treatment of EVALI is unknown, the use of corticosteroids, antibiotics, antivirals, or antifungals can be considered based on clinical suspicion. These medications should be used in accordance with published guidelines in the instances of concurrent infections such as community-acquired pneumonia or influenza. Though severity of illness varies, 96% of reported patients diagnosed with EVALI were hospitalized and 47% were admitted to the intensive care unit.
Conclusions: E-cigarette or vaping product use-associated lung injury is a relatively new and therefore likely unfamiliar phenomenon. As the vast majority of cases are encountered in the hospital setting, hospital medicine professionals are in an important position to detect and manage this patient population.