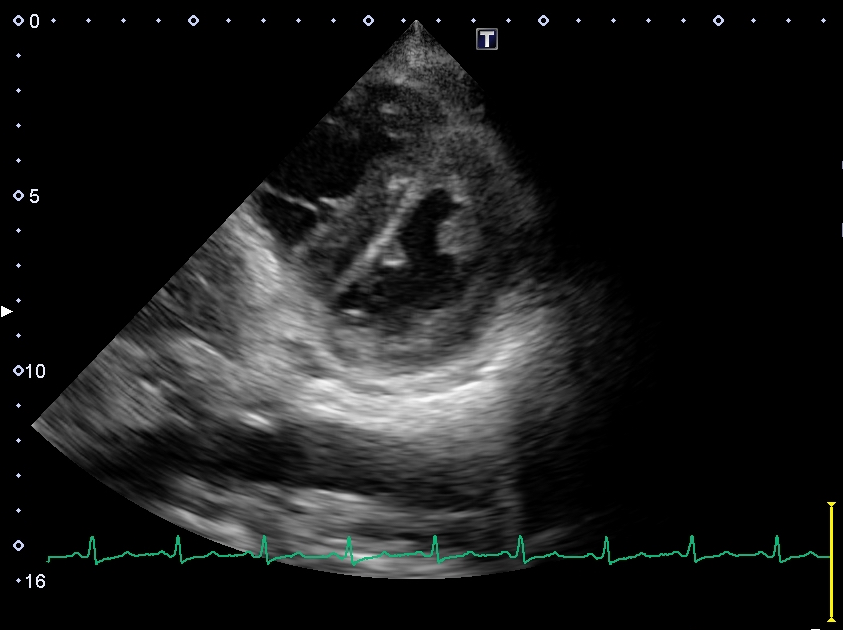
Case Presentation: A 68-year-old previously healthy woman was presented to our hospital with acute low back pain that was not triggered by any trauma. Magnetic resonance imaging (MRI) revealed a lumbar compression fracture, and she was admitted to the orthopedic department. Two days later, she developed orthopnea and hypotension, and therefore the orthopedician consulted with us about them. On further examination, she was afebrile with a heart rate of 84 beats per minute, a blood pressure of 94/54 mmHg, and a respiratory rate of 24 breaths per minute. Her oxygen saturation level was 98%, and the flow rate of oxygen was 2L per minute. Jugular venous distention and bilateral mild leg edema were detected. Her chest examination showed coarse crackles bilaterally, and her heart sound revealed an accentuated pulmonic component (IIP). The ultrasound cardiogram indicated a remarkably elevated pulmonary artery systolic pressure (PASP = 63.5 mmHg), D-shaped left ventricle (Figure 1), and bilateral pleural effusion. Laboratory data revealed a white blood count of 6.2 × 102/L; hemoglobin level, 8.4 g/dL; platelet count, 43 × 109/L; serum albumin level, 1.5 g/mL; total protein level, 10.0 g/mL; and an IgM level, 4470 mg/dL. Contrast enhanced computed tomography revealed enlargement of the right ventricle, bilateral pleural effusion, and extensive swelling of the para-aortic lymph nodes; however, pulmonary embolism and lung disease, such as chronic obstructive pulmonary disease or interstitial pneumonia, were not detected. M protein was observed on serum immunoelectrophoresis. At that time, we diagnosed pulmonary hypertension and right heart failure associated with hyperviscosity syndrome related to M proteinemia caused by Waldenstrom macroglobulinemia or multiple myeloma. We referred and transferred her to the hematology department of a general hospital. Finally, she was diagnosed with Waldenstrome macroglobulinemia based on bone marrow and lymph node biopsy and received plasma exchange therapy and chemotherapy.
Discussion: Waldenstrom macroglobulinemia is a relatively rare hematological malignancy that is known to often cause hyperviscosity syndrome due to the accumulation of monoclonal IgM antibodies. Hyperviscosity syndrome is caused by an abnormal increase in the number of blood cells or hyperproteinemia resulting in increased blood viscosity and various symptoms. The triad symptoms include mucosal or skin bleeding, neurological deficits, and visual disturbances; in addition, congestive heart failure and renal failure may also occur. Reports on pulmonary hypertension due to hyperviscosity syndrome are rarely available; however, there are a few reports on pulmonary hypertension secondary to hyperviscosity syndrome associated with rheumatoid arthritis and Sjogren’s syndrome. In this patient, right heart catheterization was not performed but the echocardiogram showed D-shaped left ventricle and high PASP characteristic of pulmonary hypertension. Her symptoms related to pulmonary hypertension and congestive heart failure rapidly improved on plasma exchange and chemotherapy.
Conclusions: Hyperviscosity syndrome associated with Waldenstrom macroglobulinemia can cause pulmonary hypertension. Acute pulmonary hypertension without any pulmonary embolism may also suggest hyperviscosity syndrome.