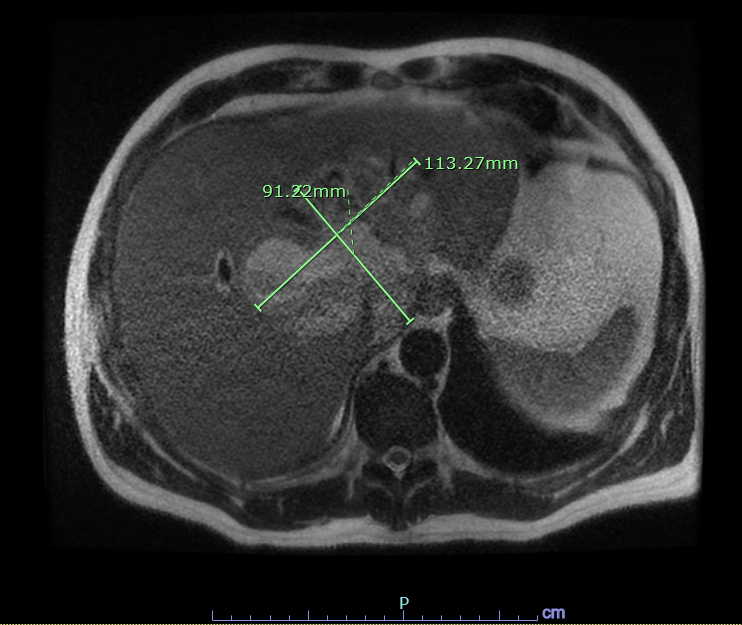
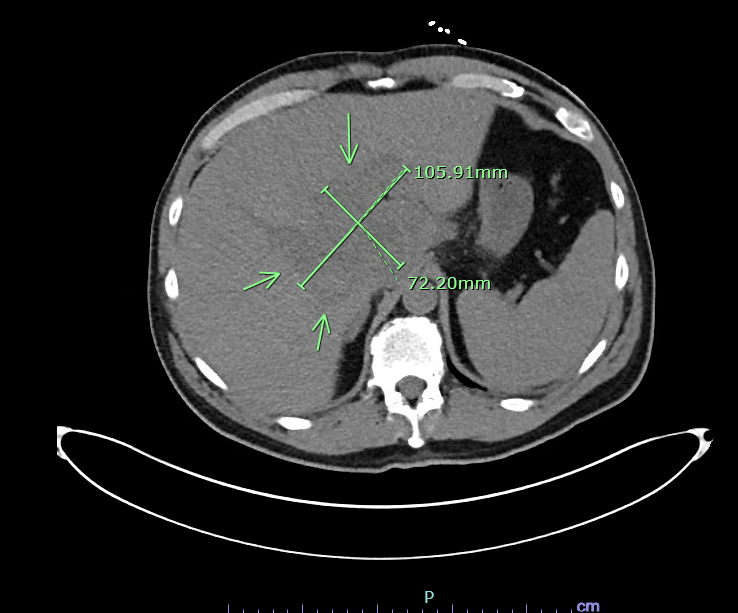
Case Presentation: A 61-year-old male with no known past medical history presented with one week history of generalized malaise and exertional dyspnea. He had undergone a dental procedure six weeks ago. He drank alcohol occasionally but denied smoking or illicit drug use. On admission, he was febrile (Temp 101.6F), tachycardic (HR 113), tachypneic (RR 25) and hypoxic requiring 2L oxygen. Physical examination was unremarkable. Initial work up was significant for leukocytosis with left shift (WBC 24.1), thrombocytopenia (platelet 104,000), elevated creatinine (5.01 mg/dL) and positive anion gap acidosis with elevated lactic acid (3 mmol/L). Liver function tests were also abnormal (ALT 479 U/L, AST 269 U/L, ALP 415 U/L, INR 1.4, albumin 2.2 g/dL, total bilirubin 2.7 mg/dL). Abdomen Imaging, namely ultrasound and CT without contrast, demonstrated findings suggestive of liver cirrhosis and a large he terogeneous area measuring 10.6 X 7.2 cm located centrally within the liver involving both hepatic lobes with some low-attenuation areas. Differentials included a benign tumor, hepatoma, metastatic lesion or abscess. Further imaging with contrast, however, was limited in view of acute renal failure. Code sepsis was initiated, and he was started empirically on broad spectrum antibiotics namely vancomycin and piperacillin-tazobactam. He was admitted to the medical stepdown unit for close monitoring. Blood cultures subsequently grew Streptococcus intermedius. AFP, CA 19-9 and CEA were normal. Echocardiogram was negative for vegetations. Antibiotics were deescalated to ceftriaxone. Repeat blood cultures showed clearance of bacteremia. Hemodialysis was initially planned but deferred as his renal function markedly improved. On the fifth hospital day, he underwent MRI with contrast which showed multiloculated central hepatic lesion measuring up to 11.3 cm compatible with an abscess which w as not amenable to IR guided drainage. He underwent laparoscopic, ultrasound guided drainage. Cultures from drainage were negative. He improved clinically and was discharged home on IV ceftriaxone for 6 weeks. Fours week later , repeat imaging in outpatient settings showed resolution of the abscess
Discussion: Pyogenic liver abscess (PLA) is a life-threatening condition that can at times be challenging to diagnose due to its nonspecific presentation or atypical radiologic findings. Timely identification is crucial in implications for treatment approach. Pyogenic liver abscess is sometimes difficult to differentiate from malignancy as its radiologic manifestations can vary with the degree of the maturation of the lesion. This often requires additional diagnostic imaging which is not without risk. As in this case, astute clinical correlation remains of utmost va lue to arrive at the correct diagnosis and treatment
Conclusions: Radiological manifestations of Pyogenic liver abscess and Hepatic malignancy can be similar and seldomly hard to differentiate , especially in setting of limited investigations. Hence , It is utmost important to emphasize on clinical findings and correlation to reach correct diagnosis for appropriate treatment and management