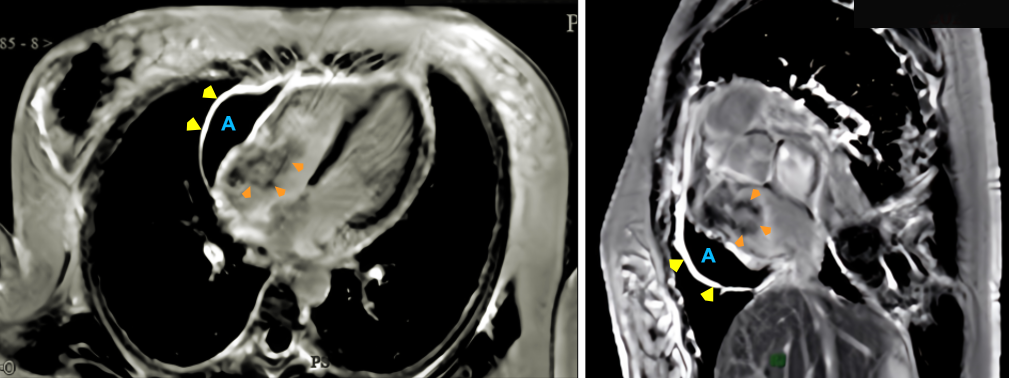
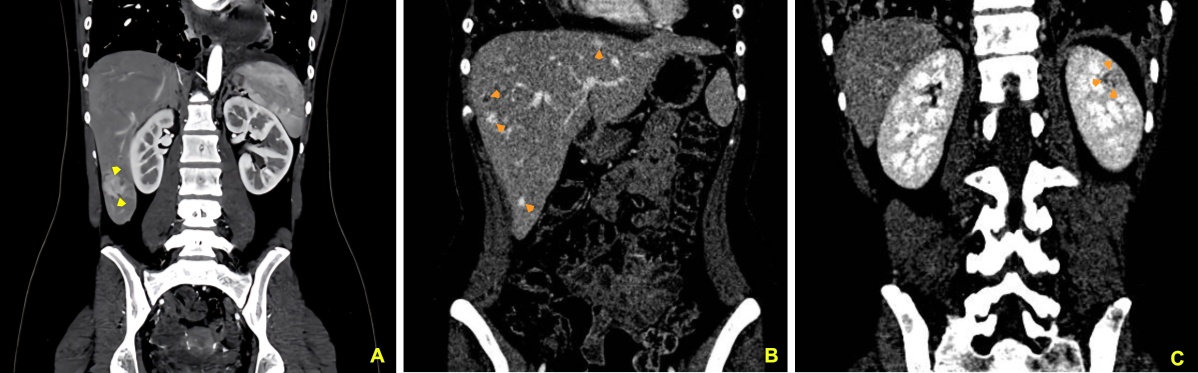
Case Presentation: A 17-year-old female presented with a one-month history of persistent dry cough, worsened by lying flat, requiring multiple pillows to sleep comfortably. Initially treated for presumed pharyngitis, her symptoms persisted, prompting further evaluation. Echocardiography revealed a large pericardial effusion with a normal ejection fraction, leading to hospital admission. Imaging studies identified a 3.5 x 4.0 cm irregular mass in the right atrium, thickened pericardial membranes, and significant pericardial effusion. Computed tomography (CT) scans also showed nodules in the mediastinum, lungs, and liver, along with a skull mass. Cardiac magnetic resonance imaging (MRI) confirmed a 5.0 x 3.0 x 4.0 cm hyperintense mass in the right atrium on T2-weighted images. Biopsy of a liver lesion confirmed angiosarcoma of cardiac origin. Despite initiating chemotherapy, the patient discontinued treatment after six months due to poor response. Follow-up imaging revealed disease progression with new lesions in the liver and left kidney.
Discussion: Cardiac angiosarcoma is the most aggressive type of primary cardiac tumor, with an incidence as low as 0.0001%. Typically arising in the right atrium, these tumors present with nonspecific symptoms such as cough, dyspnea, or pericardial effusion, which often delay diagnosis. In this case, multimodal imaging, including echocardiography, CT, and MRI, provided crucial diagnostic insights, but confirmation required histopathology. Cardiac angiosarcomas exhibit early metastatic spread, with common sites including the lungs, liver, and bones, as observed in this patient. Treatment remains challenging; surgery is rarely an option due to advanced disease at presentation, and chemotherapy and radiotherapy show limited efficacy. Heart transplantation is generally contraindicated by the presence of metastasis. Prognosis is dismal, with mean survival of 9 to 12 months post-diagnosis. This case highlights the unique challenges of diagnosing and managing juvenile-onset cardiac angiosarcoma, an exceedingly rare condition with sparse literature, emphasizing the critical need for early recognition of persistent cardiovascular symptoms in young patients.
Conclusions: This case of juvenile-onset cardiac angiosarcoma underscores the aggressive nature of this rare malignancy, marked by its rapid progression, metastatic potential, and poor response to conventional therapies. The patient’s clinical course exemplifies the diagnostic challenges posed by nonspecific symptoms and the limitations of current treatment modalities. Heightened clinical suspicion, combined with advances in imaging and early biopsy, may aid in earlier detection. However, there remains an urgent need for research into novel therapeutic approaches to improve outcomes for patients with cardiac angiosarcoma. This case adds to the limited body of knowledge, highlighting both the critical role of timely diagnosis and the pressing need for innovation in treatment strategies.