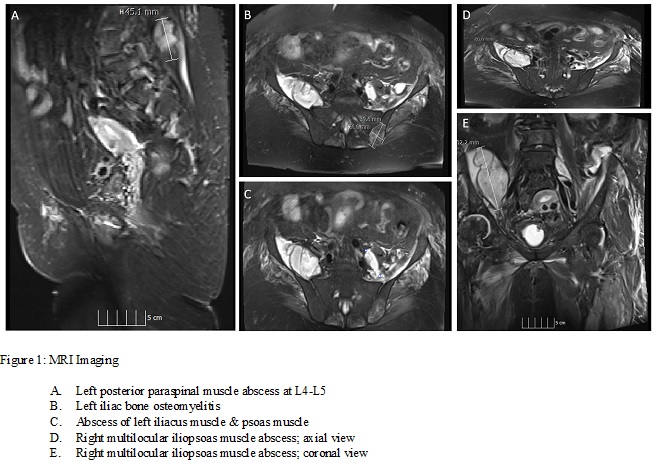
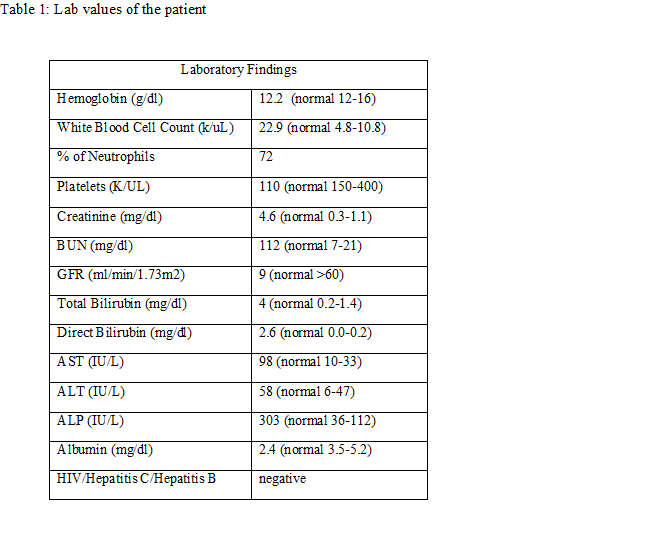
Case Presentation: An 81-year-old female with history of hypertension and hip osteoarthritis presented from rehabilitation facility with worsening right hip pain, back pain and lower abdominal pain. Laboratory work-up at the facility revealed several derangements, including elevated leukocytes. Patient was afebrile with tachycardia of 106. Pertinent examination findings included tender flexion at the right hip joint and tenderness of the suprapubic region. Laboratory findings in the hospital are summarized in table 1. The patient’s urine analysis was significant for urinary tract infection and her abdominal ultrasound was significant for cholelithiasis; hence a working diagnosis of sepsis due to urinary tract infection versus acute cholecystitis was made. Blood cultures grew methicillin sensitive staphylococcus aureus (MSSA). Patient was further worked up for infectious endocarditis and septic arthritis, which was unremarkable. CT scan of the right hip showed swelling of the right iliopsoas muscle with suspicion for an intramuscular abscess. MRI of the pelvis showed multiple intramuscular abscesses involving the iliopsoas muscles bilaterally, left obturator muscle and left posterior paraspinal muscle as well as extensive myositis and fascitis of left gluteus medius and minimus (Figure 1). Given no apparent source of multiple abscesses, the patient’s history was re-explored and revealed a recent trial of acupuncture therapy to the lower back for chronic back and hip pains. The diagnosis was revised to pyomyositis secondary to acupuncture therapy complicated by MSSA bacteremia. Interventional radiology-guided drainage was done for abscesses that grew MSSA, Escherichia coli (ESBL) and Pseudomonas aeruginosa. Patient was switched to meropenem from cefazolin, resulting in clinical improvement.
Discussion: Pyomyositis is often categorized into three clinical stages, with a gradual progression from diffuse inflammation to abscess formation (1).Stage 1: lasts from 10 to 21 days; symptoms include fever, malaise and muscle tenderness without abscess formationStage 2: characterized by abscess formation with focal complaints and worsening painStage 3: characterized by septicemia, metastatic abscesses, multi-organ dysfunction with high mortalityOur patient presented in stage 2, like the majority of cases with pyomyositis (2). Numerous studies (3), (1), (4) have indicated Staphylococcus aureus as the predominant causative organism as is found in this case. The etiology of pyomyositis is unclear but studies indicate predisposing factors include trauma, intravenous drug use, intensive exercise, malnutrition, viral and parasitic infections, immunosuppressive drugs, HIV and chronic illness like diabetes, malignancy, cirrhosis or renal disease (5), (2). Our patient revealed an interesting predisposing factor not frequently discussed in literature; the acupuncture therapy. The diagnosis of pyomyositis can be made by various noninvasive modalities including plain radiography, ultrasound, CT and MRI. The gold standard is MRI (2). Treatment for pyomyositis is based on staging. Stage 1 is treated with antibiotics, whereas stage 2 and 3 additionally require percutaneous or surgical drainage (5), (2).
Conclusions: The diagnosis of pyomyositis can be difficult to make given its variable presentation. There is limited data on this disease, which should be expanded as it is a rare but life-threatening complication of a popular therapy – acupuncture.