Background: Sleep disturbances among hospitalized adults are associated with impaired glucose regulation, increased pain intensity, prolonged length of stay, and reduced patient satisfaction. On our general medicine unit, Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) responses to the “Quietness of Hospital Environment” question consistently revealed opportunities to improve the nighttime environment. Recognizing the importance of uninterrupted sleep for patient recovery and well-being, we launched a multifaceted quality improvement initiative to reduce overnight disruptions and enhance perceived sleep quality.
Purpose: Between August 2024 and August 2025, we implemented three interventions to minimize nighttime disturbances. First, vital sign monitoring defaults were updated from q4h to q8h for clinically stable patients, reducing unnecessary overnight interruptions while preserving provider discretion. Second, patients completed the Sleep Disruption Questionnaire to identify the most disruptive nighttime activities, with early-morning lab draws emerging as a major contributor. In response, routine morning labs for patients with next-day discharge plans were rescheduled to 9 PM rather than 4 AM, later expanding unit-wide when clinically appropriate. The Richards-Campbell Sleep Questionnaire (RCSQ) was administered to measure sleep depth, latency, number of awakenings, returning to sleep, and global sleep quality (0 to 100 scale, with higher scores representing better sleep). Staff received targeted education, and patient feedback informed iterative refinements. Safety was monitored using Behavioral Emergency Response Team (BERT) and Rapid Response Team (RRT) activations.
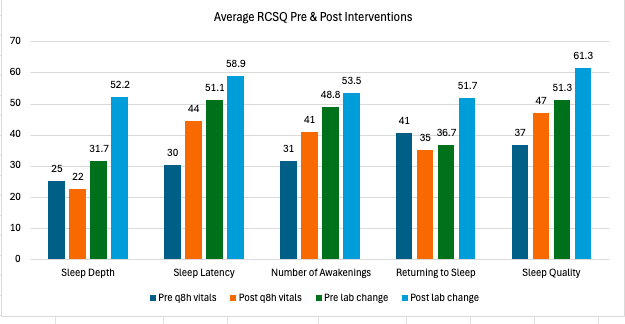
Description: Transitioning clinically stable patients to q8h vital sign monitoring resulted in improvements in multiple RCSQ domains, including increases in sleep latency (30 to 44), number of awakenings (31 to 41), and overall sleep quality (37 to 47), with mixed changes in other dimensions. Following the lab-timing change, sleep depth improved markedly from 31 to 52, along with similar improvements across additional RCSQ domains. HCAHPS “Quietness of Hospital Environment” scores increased from 0% pre-intervention (June 2024) to 46% after the vital sign change (September 2024) and 75% after the lab timing change (August 2025). BERT and RRT activations remained stable throughout the intervention period, indicating no compromise in patient safety.
Conclusions: A multimodal, patient-informed approach to nighttime care—centered on reducing vital sign frequency for stable patients and shifting lab draws earlier in the evening—resulted in substantial improvements in patient-reported sleep quality and HCAHPS quietness scores without increasing emergency response activations. These findings demonstrate that targeted operational adjustments can meaningfully enhance inpatient restfulness while maintaining clinical safety.