Background: Effective communication affects cancer management and outcomes and is particularly essential in the last year of life when medical complexity peaks. In the last decade, adoption of telemedicine and other advances may have affected patient experience and communication effectiveness. The purpose of this study is to assess racial disparities and trends in patient experience and communication satisfaction among cancer patients in the last year of life.
Methods: We used the Surveillance, Epidemiology and End Results (SEER) cancer registry data linked with Consumer Assessment of Healthcare Providers and Systems (CAHPS) patient survey data. Inclusion criteria included: a) completion of the CAHPS survey between 2000-2019, b) aged ≥ 66 years at the time of survey completion c) completion of survey within the last year of life d) and diagnosed with breast, prostate, lung, colorectal, uterine, skin, kidney, bladder, pancreatic and/or ovarian cancer. Patient characteristics are reported as weighted mean (standard deviation (SD)) or percentage (95% confidence interval (CI)). Chi square test or analysis of variance were used as appropriate to assess statistically significant differences between groups. We used multivariable linear regression models to assess racial disparities in single item (“rate MD,” “rate care,” “MD listen” and “MD explain”) and composite measure (“getting care quickly,” “getting needed prescription drugs,” “getting needed care,” and “doctor communication”) ratings. We used multivariable logistic regression models to assess differences in ratings for patient surveys completed between 2000-2011 and 2012-2019, respectively. All analyses were conducted with survey weights accounted for.
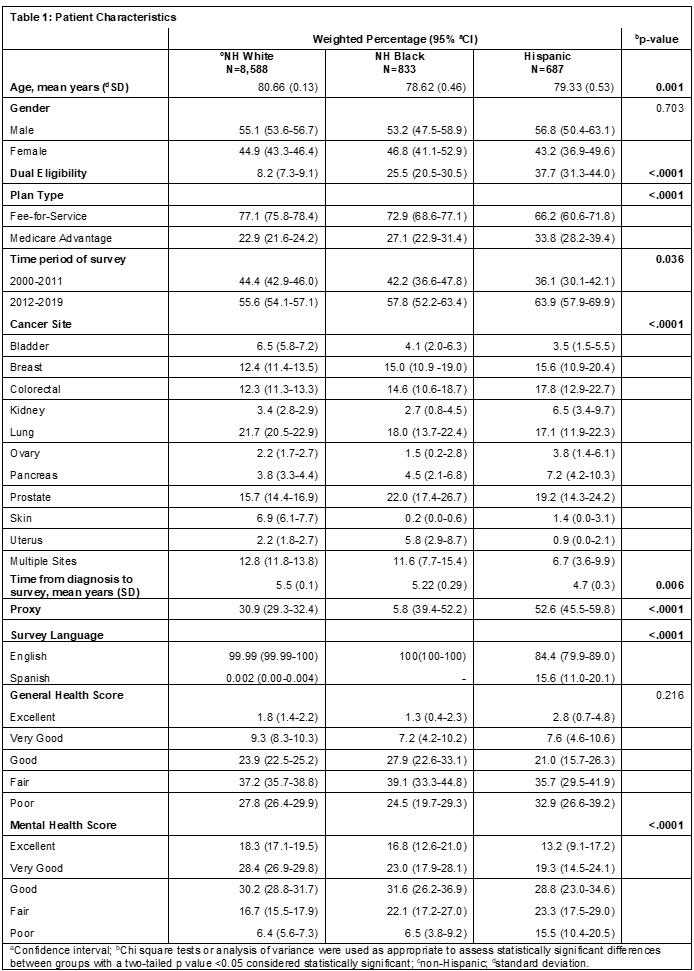
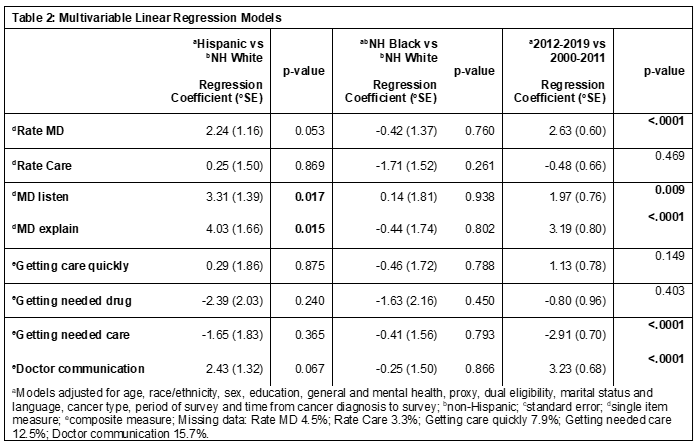
Results: A total of 10,108 patients met inclusion criteria. Non-Hispanic Black patients were younger at the time of survey completion compared to other groups. Hispanics were more likely to be dually eligible, to have a proxy complete the survey and to complete the survey in Spanish. The most common cancer types were lung, prostate, colorectal, and breast. In multivariable logistic regression models, we found Hispanic patients rated “MD listen” and “MD explain” significantly better than non-Hispanic White patients. There were no differences in ratings between non-Hispanic Black and non-Hispanic White patients. Surveys completed in 2012-2019 had improved ratings for “rate MD,” “MD listen,” “MD explain,” and “doctor communication” but a worse rating for “getting needed care” compared to survey ratings reported in 2000-2011, respectively.
Conclusions: Differences in ratings between Hispanic and non-Hispanic White patients could have been due to higher rates of proxy completion for Hispanic patients. There were no significant differences between non-Hispanic Black and non-Hispanic White ratings despite known differences in survival and other outcomes. Ratings for multiple measures including “MD listen” for surveys completed between 2012-2019 were significantly better compared to ratings from 2000-2011. This could be due to shifting trends in technology use including increased patient access to medical records and advance care planning among others. However, “getting needed care” was significantly lower. This could be due to improved cancer survival and more life years with disability requiring more care at the end of life. Limitations of this data include limited sampling of minoritized patients and some missing data.