Background: Hospital admissions among nursing home residents with Alzheimer’s Disease and related dementias (ADRD) are burdensome, expensive, and provide limited clinical benefits. Compared to other patients, those with ADRD are more likely to experience adverse events, such as delirium, urinary infections, pneumonia, and functional decline. Research on nursing home residents has focused on the consequences of hospitalizations after their hospital stay, or specific adverse outcomes, such as rates of feeding tube insertions, lengths of stay, or mortality. Our objective was to comprehensively describe the in-hospital experience of nursing home patients with ADRD.
Methods: We analyzed charts of patients aged 18+ years with an ADRD diagnosis ICD code who resided in a nursing home and were transferred to a hospital from January 2013 to July 2023. One randomly selected hospitalization per patient was included in the analysis. We used R 4.4.1 to conduct the descriptive analysis.
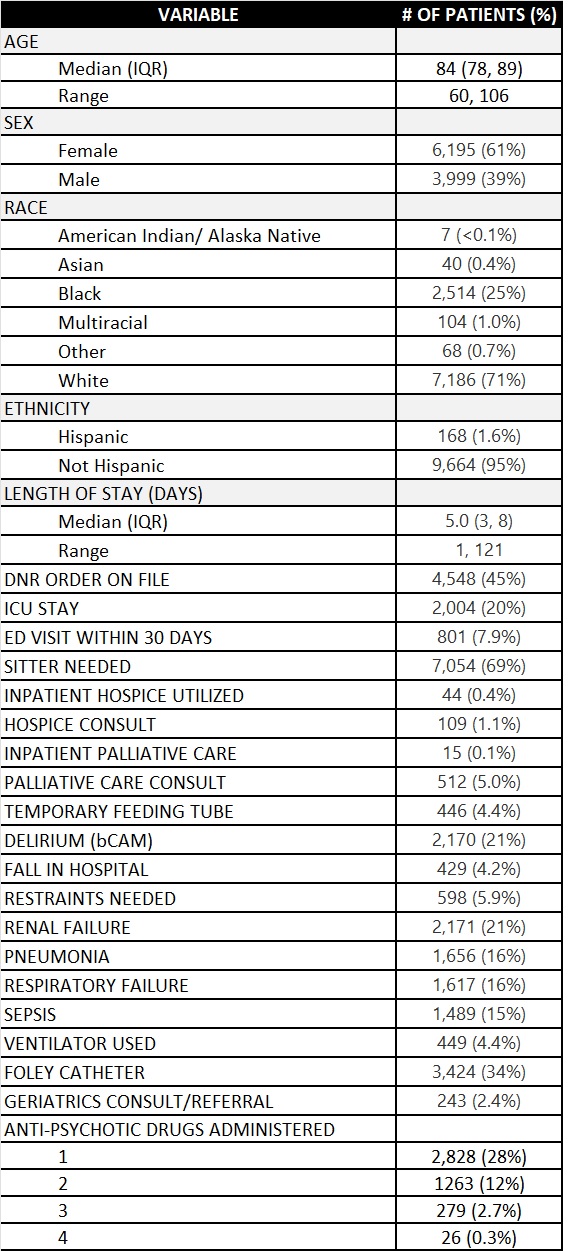
Results: Of 10,195 patients, the median age was 84 years, 71% were white, 25% black, 61% female, and the median length of stay was 5 days. During the hospitalization, 69% needed a sitter, 34% had a Foley catheter, and 4% had a feeding tube. 21% had delirium, 6% were put in restraints, 4% experienced a fall, and at least 1 anti-psychotic drug was administered to 28% of patients. 21% had renal failure, 16% respiratory failure, 16% pneumonia, and 15% sepsis.One-fifth (20%) of patients were sent to the ICU and 4% received mechanical ventilation; only 1% had a hospice consult, 0.4% had inpatient hospice, 5% had a palliative care consult, 0.1% inpatient palliative care, and 2% had a consult/referral to geriatrics. Less than half (45%) had a DNR order.More than 1/3 (34.8%; 3,546) of patients died within 6 months. Of these, 61% had a DNR order, but only 2.3% received a consult to hospice; 1.1% had inpatient hospice; 9.4% had a palliative care consult; and 0.3% had inpatient palliative care.
Conclusions: Nursing home patients with ADRD who were transferred to the hospital often endured distressing experiences, but rarely were referred to hospice or palliative care, despite high mortality. Patients and their family members should be informed about the hospital experience and offered hospice and palliative care services when appropriate. Given hospitalists’ limited time and lack of communication training about palliative care or hospice, systemic workflow changes should be implemented to prioritize these complex consultation decisions.