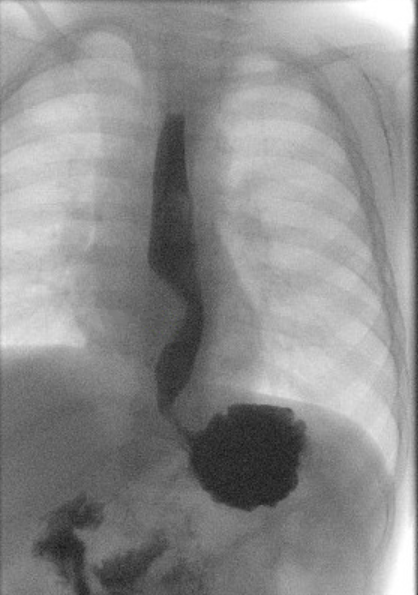
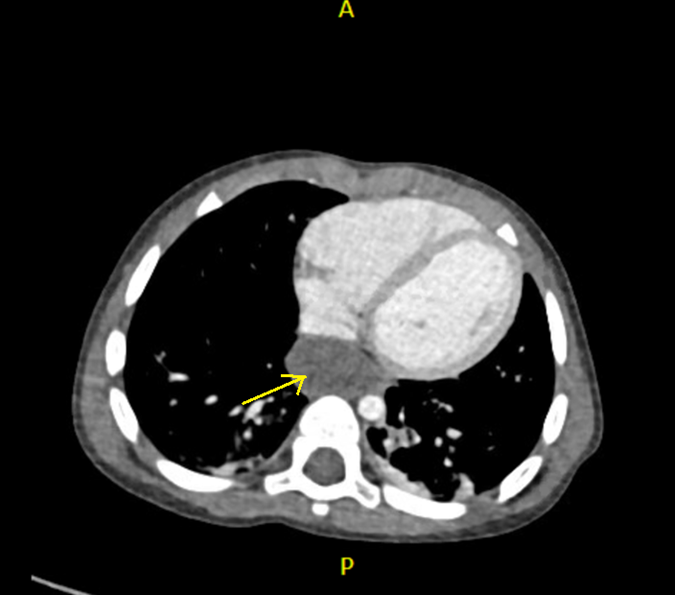
Case Presentation: A 16-month-old male with a history of reactive airway disease presented to clinic for evaluation of vomiting for four months. He had a history of chronic cough and had been started on acid suppression for gastroesophageal reflux but did not have any improvement in symptoms. His physical examination was unremarkable. He also had intermittent episodes of choking, and an esophagram was performed which showed a cystic indentation of the lower esophagus. Computed tomography of the chest showed a well-circumscribed esophageal duplication cyst. He underwent open thoracotomy for resection of the duplication cyst and did well post-operatively with complete resolution of his symptoms. The pathology showed a 2.5 x 2 x 0.5 cm muscular cyst with ciliated respiratory epithelial lining, consistent with an esophageal duplication cyst.
Discussion: Esophageal duplication cysts are rare congenital malformations that result from abnormalities in the division of the embryonic foregut. The incidence is about 1 in 8200 patients and is found predominantly in children. Diagnosis is established by two years of age in more than 80% of patients. Most esophageal duplication cysts are found in the inferior mediastinum and lengthen in the thoracic region of the esophagus. The differential diagnosis includes lipoma, leiomyoma, gastrointestinal stromal tumor, pericardial cyst, and cystic hygroma. The diagnostic criteria for esophageal duplication cyst includes a mass that is attached to or within the esophageal wall, covered by two muscle layers, and lined by squamous, columnar, cuboidal, pseudostratified, or ciliated epithelium.Symptoms may result from compression of surrounding structures and include dysphagia, epigastric pain, and respiratory distress. Computed tomography and magnetic resonance imaging are the preferred imaging modalities, although endoscopic ultrasound has also been used. Treatment is by surgical resection, generally through a thoracoscopic approach. Prophylactic removal may often prevent potential complications including infection, cyst rupture, and malignancy. Progression to malignancy is extremely rare. Surgical resection is indicated for all symptomatic lesions and can be considered for asymptomatic cysts. However, surgery for asymptomatic cysts can lead to long-term complications such as heartburn and reflux esophagitis.
Conclusions: Esophageal duplication cysts are rare congenital malformations that develop from abnormalities in the division of the embryonic foregut. The clinical presentation may mimic gastroesophageal reflux or respiratory disease. Appropriate imaging modalities including upper GI series, computed tomography, or magnetic resonance imaging can help to establish the diagnosis.