Background: Current Infectious Diseases Society of America (IDSA) practice guidelines for skin and soft tissue infections (SSTIs) recommend against obtaining blood cultures for typical presentations of cellulitis. The guidelines only recommend cultures for those patients with malignancy on chemotherapy, neutropenia, severe cell-mediated immunity, immersion injuries or animal bites. Our institution has no protocol for guiding when to obtain blood cultures in patients presenting to the emergency department (ED) with SSTIs. The objectives of this study were 1) to determine which patient characteristics were predictive of blood cultures obtainment and 2) to identify the yield of blood cultures obtained for SSTIs among patients hospitalized in an observation unit from the ED.
Methods: A retrospective chart review was performed to identify patients admitted to the UNC Observation Unit from the ED with a diagnosis of SSTI utilizing International Classification of Diseases, ver. 10 codes. We recorded demographics, initial lab results and vital signs while in the ED. We also recorded whether blood cultures were obtained on presentation and the results of any obtained cultures. We performed univariate and multivariate analyses to determine which demographic and clinical characteristics were predictive of obtaining blood cultures in the ED.
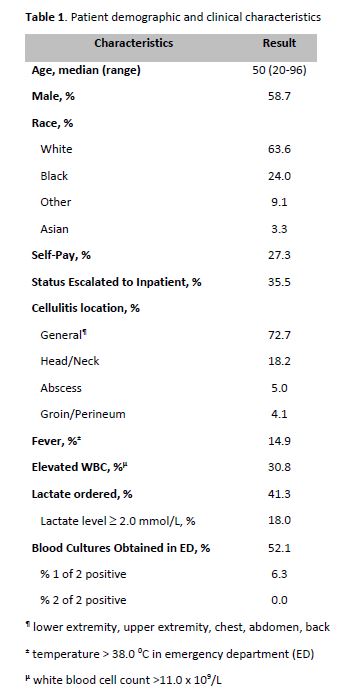
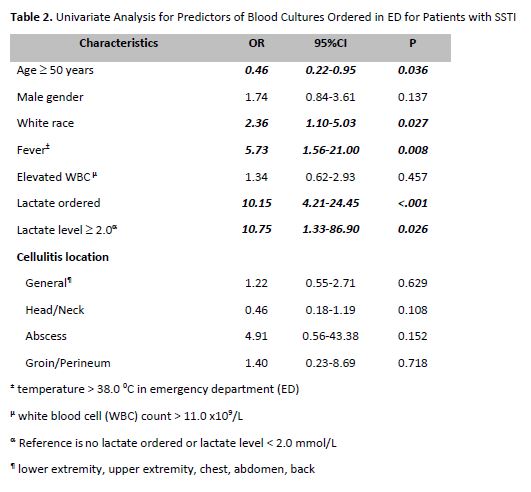
Results: We identified 121 patients hospitalized in our observation unit from the ED over a 12 month period with a diagnosis of SSTI (Table 1). Of these patients, 63 (52.1%) had blood cultures obtained in the ED. In univariate analysis, factors predictive of having blood cultures obtained were age > 50 yrs, white race, fever, lactate ordered and lactate >2.0 mmol/L (Table 2). In multivariate analysis, white race (OR 3.13, 95% CI 1.29-7.56) and fever (OR 5.25, 95% CI 1.30-21.26) remained predictors. Among patients with cultures drawn, four (6.3%) had positive cultures. Two patients (3.2%) grew species identified as contaminants. Two patients (3.2%) grew species treated as pathogens. One of these patient was receiving chemotherapy for invasive breast malignancy, meeting IDSA guideline criteria for culture, and grew group B Streptococcus. The other patient had been in the hospital the previous day, but returned with an infected IV site and grew methicillin sensitive staph aureus. Both patients met criteria for inpatient status.
Conclusions: Blood cultures were ordered in over half of patients hospitalized with SSTI from the ED to our observation. Fever and white race were predictors of blood cultures being drawn, with the latter potentially reflecting the growing rates of intravenous drug use among that demographic in our state. There was also correlation between ordering lactate and blood cultures in the ED, likely due to recent implementation of a sepsis order set.