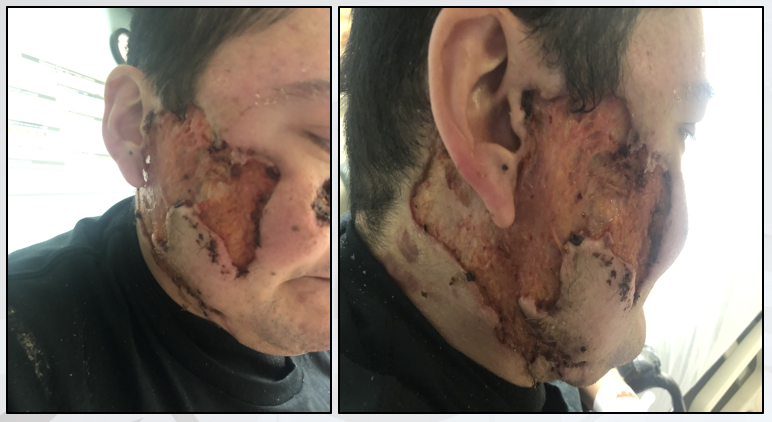
Case Presentation: A 36-year old male with a history of paraplegia secondary to a motor vehicle accident and long-standing polysubstance abuse presents to the ED for worsening facial wounds that first appeared two years ago. The patient states the most recent lesion on the upper back appeared two months ago and was preceded by cocaine use. The patient reports subjective fevers over the past several days. Vital signs upon admission include a temperature of 98.0, heart rate 90, respiratory rate 18, blood pressure 185/94, and BMI 28. Physical examination reveals dry necrotic skin lesions on the face, upper and lower back, and extremities in various stages of healing. Crepitus and fluctuance are absent. Laboratory testing reveals an elevated WBC count of 18.7 with a left shift. Antibody testing for ANCA and wound cultures are negative. A skin biopsy from a lesion during a previous hospitalization one year prior to presentation revealed necrotic abscess tissue with significant fibrosis. These lesions were previously attributed to pyoderma gangrenosum and unsuccessfully treated with prednisone and doxycycline. During the current hospitalization, a dermatology consult suggested the findings were instead consistent with a vasculopathy secondary to levamisole-adulterated cocaine. Laboratory testing from previous hospitalizations revealed a urine drug screen that was positive for cocaine use, corroborating the patient’s statements made during the current hospitalization and solidifying the diagnosis.
Discussion: Levamisole is an anti-helminthic medication commonly used as an adulterant added to cocaine in certain regions in the southern United States. The use of levamisole in cocaine has been detected since the early 2000’s, and the Drug Enforcement Agency estimates approximately 69% of seized cocaine contains a considerable amount of levamisole, highlighting an urgent need to investigate issues related to this adulterant. Exposure to this adulterant can cause a devastating small-vessel vasculitis that can result in significant skin necrosis and facial disfigurement termed levamisole-induced necrosis syndrome (LINES). Patients presenting with severe necrotizing skin lesions can raise concern for infectious and autoimmune disease processes. Unfortunately, inadequate history-taking can lead to erroneous management and lead to consistently unresolved problems such as the case of this patient, who has been hospitalized multiple times with lesions attributed to other more common etiologies. Identification of cocaine use as the cause of the patient’s lesions led to the cessation of both the patient’s consumption of cocaine and further lesion development. Urine drug screening in these patient populations may help ascertain a cause of necrotizing skin lesions that may have been otherwise overlooked during the initial evaluation.
Conclusions: In patients presenting with necrotizing skin lesions, early consideration of cocaine abuse and appropriate social history taking can help ascertain the etiology of the lesions. A urine drug screen may uncover illicit drug abuse, but the importance of building a trustful rapport with patients during clinical encounters can be critical in medical decision-making, particularly in cases of levamisole-induced vasculitis and necrosis syndrome (LINES). The substantial use of recreational cocaine consumption in the United States highlights the importance of rapid detection of this serious complication.