Background: Handoffs are critical for conveying essential information about the patient’s care, yet they often lack structure and completeness, which increases the risk of adverse events and medical errors. Patients with LEP are especially vulnerable due to communication barriers, which can exacerbate disparities in care quality and outcomes. Despite the rising number of patients with LEP, there is limited research addressing the challenges of handoffs for this population. The objective of this study was to identify gaps and opportunities for improvement in handoffs of patients with LEP, focusing on developing best practices to enhance safety and care quality.
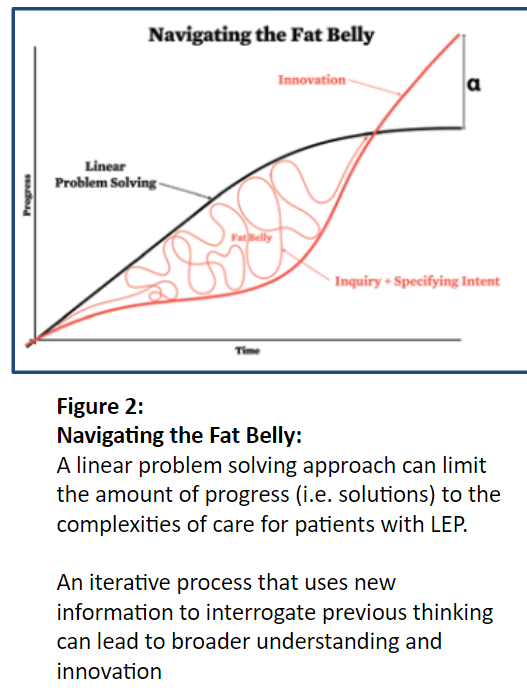
Methods: This study is part of a health equity initiative funded by the Robert Wood Johnson Foundation and was conducted within the Division of Hospital Medicine (DHM) at a large urban academic medical center. The project was designed in collaboration with systems designers from the Rhode Island School of Design (RISD) and hospitalists. From November 2022 to June 2024, 24 end-of-service handoffs were observed by two hospitalists and two medical students. Data were collected through field notes using a standardized form, Guide for Observing Handoffs. Key sections such as language needs, cultural considerations, health literacy, and family involvement were informed by previous hospitalist input through surveys. We used an iterative, abductive research approach to interpret the handoff observations and formulate themes around handoffs for patients with LEP. In Zoom meetings, a multidisciplinary panel of two hospitalists, two medical students, and two design experts from RISD discussed findings using an established Framework for Analysis. The panel agreed upon sixty-eight themes, after which the themes were narrowed to handoff recommendations for patients with LEP.
Results: The analysis revealed significant variability in handoff practices, with most providers not mentioning LEP status or associated challenges during handoffs. Language needs and cultural considerations were infrequently mentioned. No overt biases were identified, but the lack of focus on LEP issues raises concerns about missed opportunities to optimize care for this vulnerable group. Furthermore, inconsistent discussion of health literacy and family involvement was observed, which could lead to communication gaps and adverse events. These findings suggest that current handoff practices do not adequately address the needs of LEP patients and that standardized handoff protocols may be beneficial.
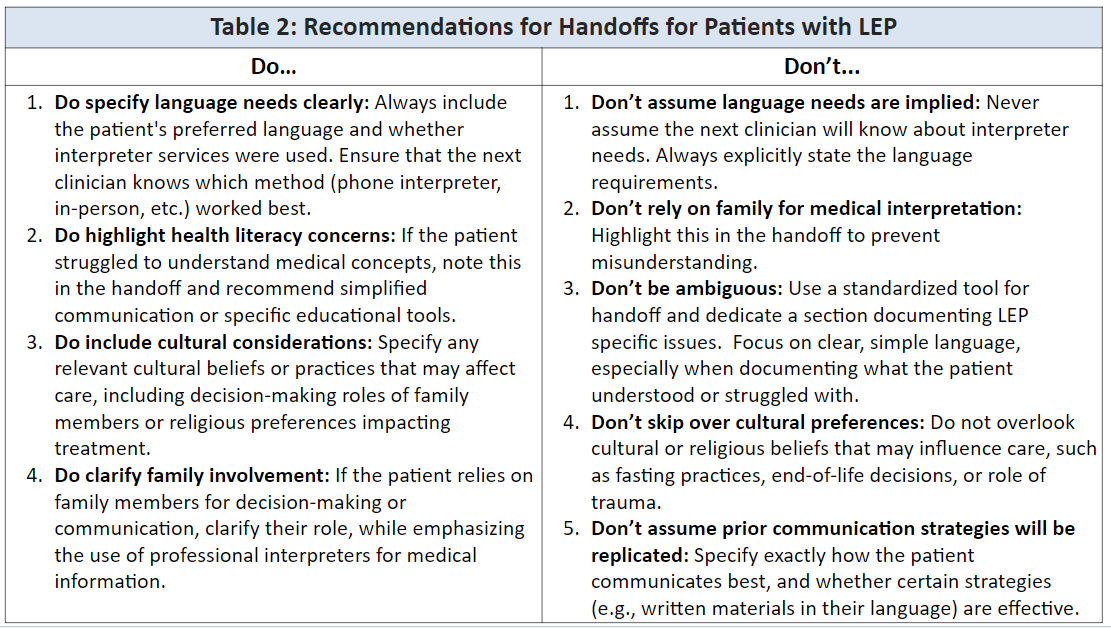
Conclusions: Our findings underscore the gap between the needs of hospitalists during handoffs and the actual handoff practice when discussing patients with LEP. There is a need for consistency and standardization, including discussing language preferences, interpreter use, and cultural factors that impact care. By integrating these elements into routine handoffs, providers can promote continuity, reduce the risk of communication failures, and improve patient safety. Limitations include reflexivity bias as the novel methodology was designed and enacted by the research team. Future research should evaluate the impact of standardized handoff protocols on patient outcomes, particularly reducing medical errors and improving care coordination. These best practices have the potential to significantly enhance care for patients with LEP, and their integration into clinical practice may lead to safer, more equitable care transitions.