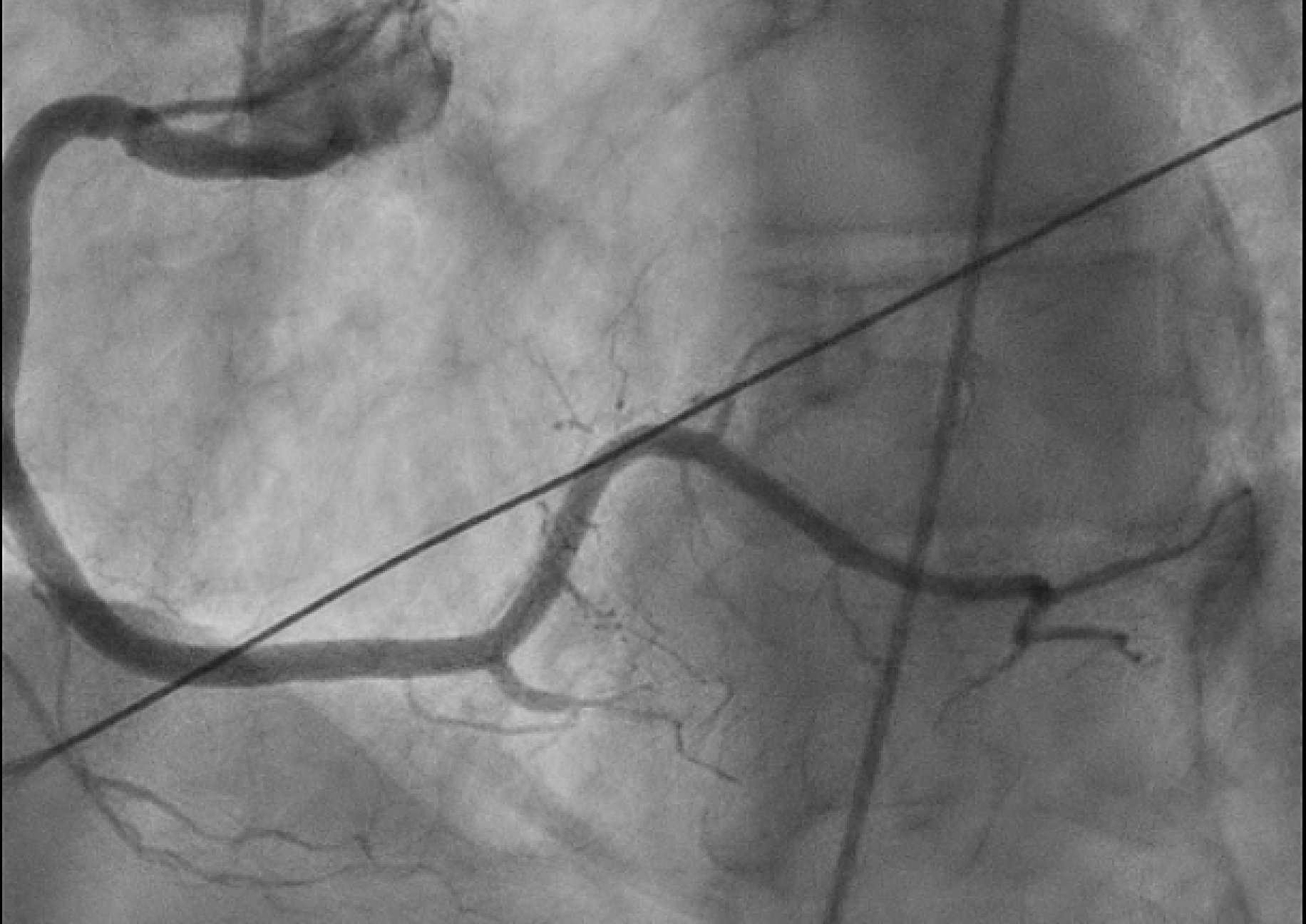
Case Presentation: We have a 63 year old female with a history of spontaneous coronary artery dissection (SCAD) of the left anterior descending artery (LAD) 2 years prior that was found on a left heart catheterization after she presented to the ER with a complaint of chest pain with associated dyspnea. On a physical exam, the patient was in distress with an unremarkable cardiopulmonary exam. EKG was significant for ST elevations in leads II, III, and aVF consistent with an inferior STEMI. She was urgently taken for coronary angiography that showed severe (90%) stenosis of the long segment branch of the right posterior descending artery (RPDA) with pruning of distal branches consistent with SCAD. Initially, the artery had TIMI 1 flow (figure 1) but improved to TIMI 2 flow with intracoronary nitroglycerin administration (figure 2). No increased tortuosity was noted on the angiogram. Echocardiogram done showed an ejection fraction of 60-65%. Her risk factors for metabolic syndrome were optimized. She was monitored closely in the ICU overnight on nitroglycerin infusion with management of chest pain. She was counseled on the benefits of tobacco smoking cessation and the risks of possible SCAD recurring with continued smoking.
Discussion: SCAD is a significant cause of acute coronary syndrome with patients presenting with acute chest pain. SCAD has a high rate of recurrence of 29% within 2-3 years and 11% within 10 years. Recurrent SCAD typically occurs in a different anatomical site than the initial occurrence and can present itself as a myocardial infarction, ventricular arrhythmia, or cardiogenic shock. Current research indicates that medical management with a beta blocker and controlling hypertension should decrease the risk of recurrence of SCAD. Studies also show that increased tortuosity of the coronary arteries increase risk of recurrence. However this patient was taking a beta blocker, had controlled hypertension, and no tortuosity of her coronary arteries seen on angiograms. There is also an unclear association between smoking and recurrence of SCAD based on current literature review.
Conclusions: This case is reported to emphasize a need for further risk stratifications to predict the recurrence of SCAD. Particularly, into the association with smoking seeing that our patient was on goal directed medical therapy yet still suffered from SCAD recurrence. Data is clear in optimizing goal directed medical therapy early on in treating the manifestations of metabolic syndrome including hypertension, diabetes, and heart disease which lead to less hospitalizations. Recurrent SCAD truly is a phenomenon for which medical therapy still may not prevent acute coronary events.