Background: The hospitalist service at this large Academic tertiary center has a length of stay index that is longer than expected. Despite improvements in multi-disciplinary rounds and co-locating patients on a geographical units, improvements in length of stay slowed. Interviews of hospitalist physicians indicate that there are frequent delays in procedures, imaging and consult recommendations. However, the hospitalists have no mechanism to alert administrators about these delays and they then expend extra time to work around these delays.
Purpose: By creating an electronic red flag alert for each delay accompanied by a brief explanation and organizing an administrative rapid action team to quickly address these delays we predicted we could reduce delays and reduce the average length of hospital staySpecific Aims – 1. Create an electronic notification system within our EMR that could be activated by our hospitalist physicians and/or case managers.2. Create an administrative team to intervene to shorten process delays.3. Create a series of communication channels for each category of process delay to assure timely responses to patient delays.4. Reduce process delays and reduce the average length of stay in the intervention group.
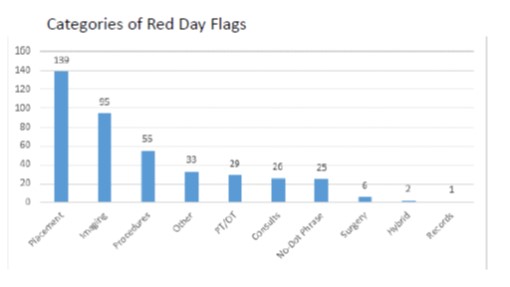
Description: We created a visual control – Red Day Flag to notify an administrative team of a process delay. The red day flag can be entered by the physician, nurse or case manager involved in the care of the patient by going to the EPIC and clicking on the FYI icon (upper right-hand corner of the standard EPIC patient face page) and enter search for “Red Day”. The Red Day Flag is accompanied by a comment box where the cause of the delay can be entered.An administrative team then could download the report daily to take action on the delay. Additionally, specific areas (procedures, imaging) can also access the report in the EMR to develop internal processes to address delays.
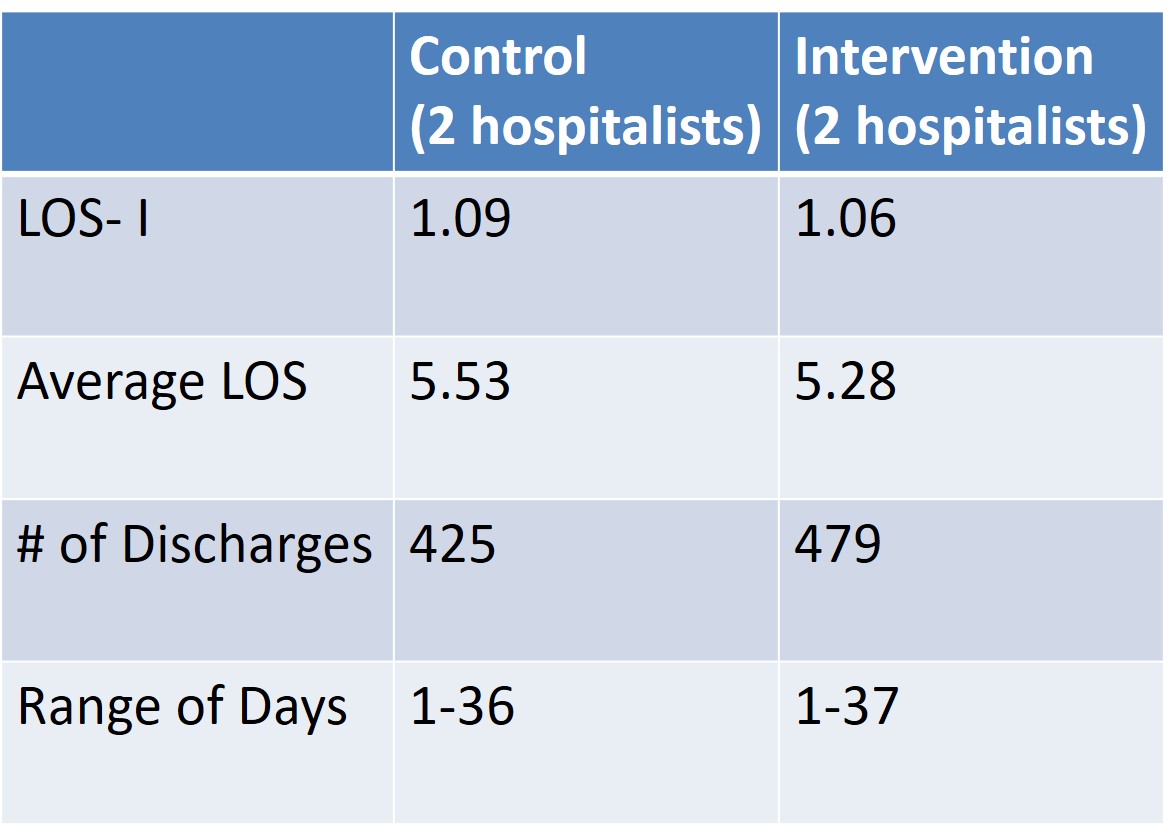
Conclusions: The study period was from 6/6/18 to 9/30/18. In thecontrol group, there were 425 discharges with an ALOS of5.53 and a LOS index of 1.09. In the intervention group,there were 479 discharges with an ALOS of 5.28 and a LOSof 1.06. While the LOS index only decreased by .03, itshould be noted that the intervention group was able toadmit and discharge an additional 50 patients comparedto the control group for the same time frame. Additionally,we were able to categorize areas of systems delays such asMRI imaging, endoscopy and subspecialty consults. Wewere then able to work with key stakeholders to improvesystems of care. This is the pilot stage of the study. Phase 2is to expand the activation of the Red flag to morephysicians so that we can have a larger number of patientsin the intervention group. As a balancing measure,readmission rates were followed and actually decreasedfrom 17.7 % to 15.2% for the entire ward where theintervention was piloted. In addition to improving systemsand reducing delay, the visual control allowed thephysicians and administrators to work together towards acommon goal. Adding the Red flag did not add additionaltime to the physicians’ work and the physician was able tofocus on patient-centered care as opposed to calling andcoordinating to intervene on a delay. This is especiallyimportant as we focus to reduce administrativeburden, improve time at the bedside for both patient andphysician satisfaction.