Background: Perioperative medicine focuses on providing patient-centered care throughout the pre-operative and post-operative periods. This area of medicine is critical given its potential to limit complications, improve post-operative outcomes, and decrease the duration of hospitalization after surgery. In recent years, perioperative medicine teaching during residency has become a requirement by The Accreditation Council for Graduate Medical Education/American Board of Internal Medicine. This has led institutions to develop and implement their own curricula(1)(2)(3). However, there is lack of standardization and evaluation data for perioperative medicine curricula. The perioperative medicine curriculum at our institution was redesigned recently. We present educational strategies and evaluation data for our redesigned curriculum.
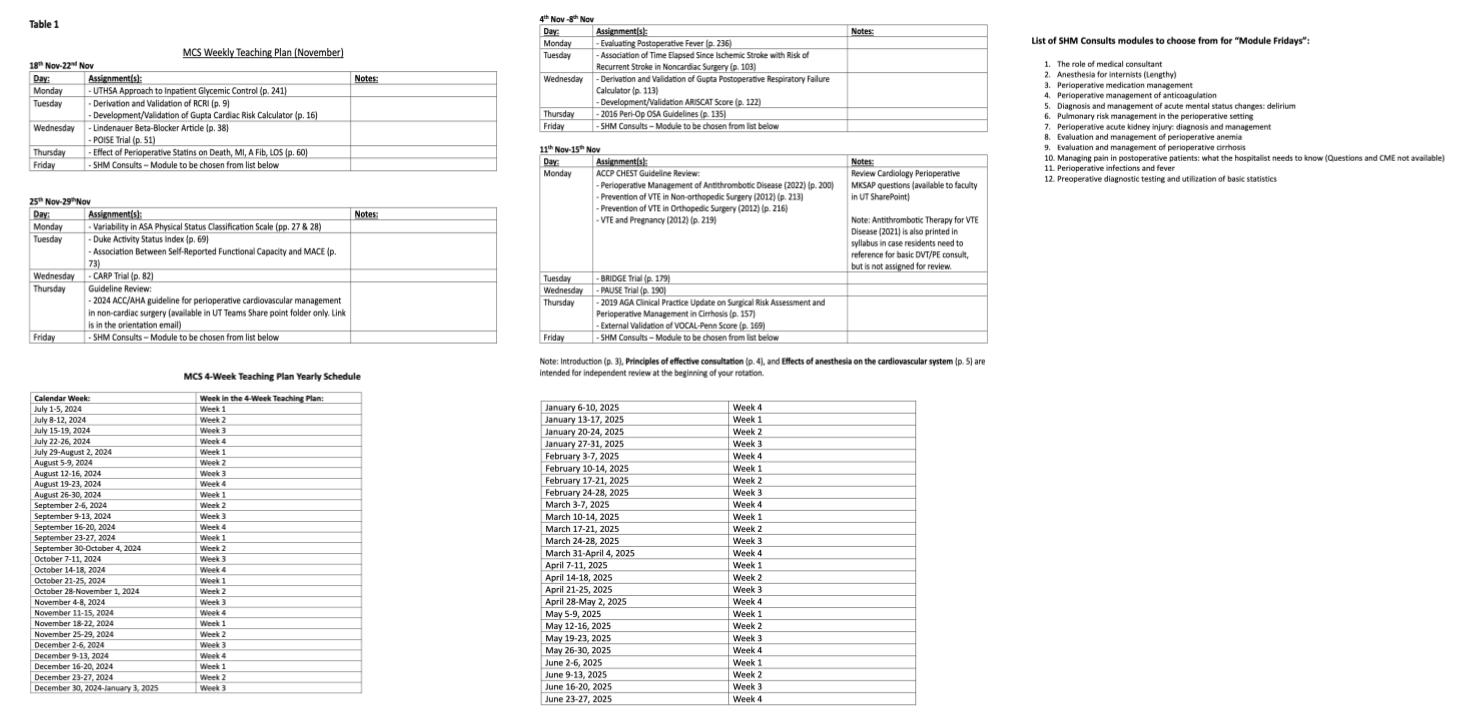
Methods: Internal medicine residents at the University of Texas, San Antonio rotate at University Hospital (1000 beds) and the Audie L. Murphy Veterans Hospital (650 beds) as part of their perioperative medicine rotation. We provide inpatient consulting services to neurosurgery, orthopedics, plastic surgery, ENT, urology, gynecology oncology, acute care surgery, general surgery and surgical oncology between the two hospitals. Before the redesign, the didactic portion of our perioperative medicine curriculum included daily perioperative faculty-led sessions covering critical appraisal of the perioperative medicine literature. Articles were printed and condensed in a “Bluebook” and copies provided to residents at orientation. We followed Kern’s 6 steps of curriculum design. Curriculum redesign included updating the “Bluebook” with recent perioperative medicine articles. We also added Society of Hospital Medicine’s (SHM) online perioperative medicine modules to our curriculum. Daily faculty led critical appraisal was continued with the addition of faculty led “Module Fridays” on a weekly basis. We also assigned specific days to specific topics in the redesigned curriculum (Table 1).Surveys were distributed over the course of one year from July 2023-June 2024. Residents received a questionnaire at the start of their 4-week perioperative medicine rotation in which they reported their confidence level with topics covered in the redesigned curriculum. At the end of their rotation, the same survey was re-sent to each resident. The study received a total of 12 pre-survey and 8 post-survey responses.
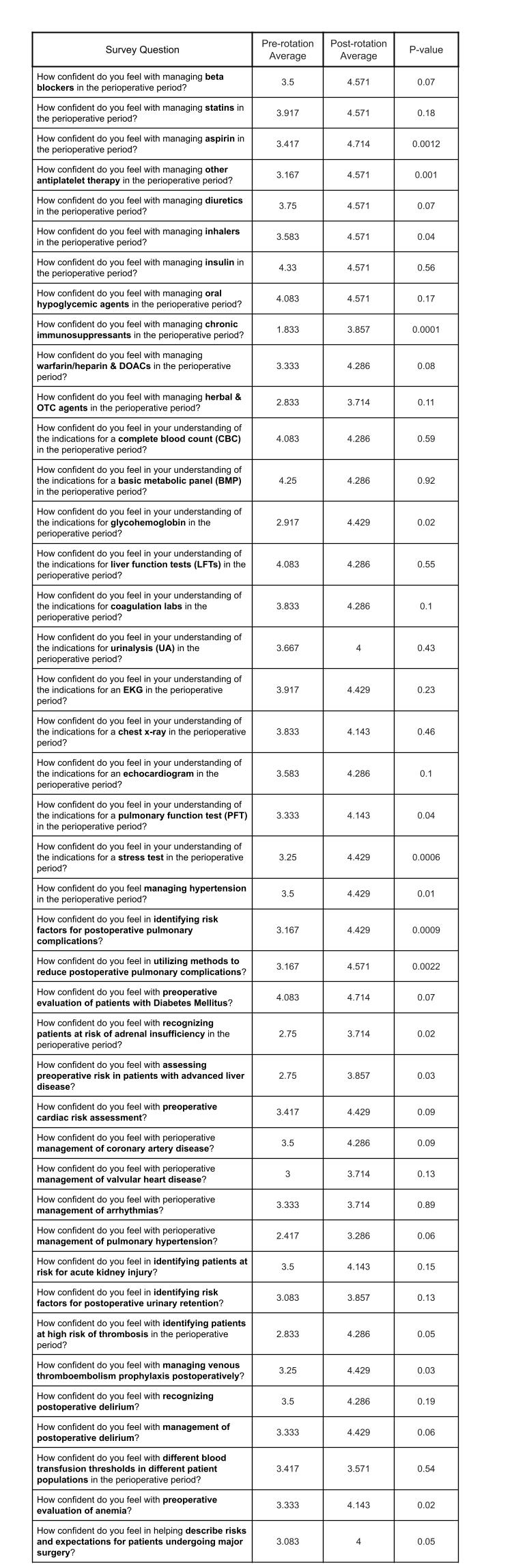
Results: Trainees reported increased understanding of perioperative management of medications, testing, and chronic medical conditions as hypertension, diabetes, anemia, liver disease, coronary artery disease and valvular heart disease. They also reported increased understanding of diagnosing and managing specific problems related to the perioperative period as acute kidney injury, urinary retention, delirium, and management of venous thromboembolism prophylaxis. This improvement was seen in all 42 questions on the pre-post survey. There was statistically significant improvement in 15 out of 42 questions (Table 2). The study was underpowered to detect a difference across all questions due to the low survey response rate.
Conclusions: A redesign of our perioperative medicine curriculum with structured assignment of updated peri-operative medicine articles and incorporation of SHM modules was well received with residents reporting increased confidence levels across a wide range of peri-operative medicine topics.