Background:
Cardiac telemetry allows hospitalists to monitor for dangerous arrhythmias. The American Heart Association has published indications on which patients are likely to benefit from telemetry. The Society of Hospital Medicine highlighted this issue through the Choosing Wisely campaign and recommended protocols to limit overuse of telemetry. Our hospital does not require an indication to initiate telemetry, lacks a protocol for discontinuation, and has a high percentage of patients on telemetry without an order.
Methods:
Targeting a unit with a majority of medicine patients, we collected baseline data over two days in early 2015, including whether patients were on telemetry and presence of an order. Next, we presented this project in a best practices format to faculty in the Division of Hospital Medicine and nursing leadership to define the problem and highlight appropriate use. We recruited a unit-based nurse manager to act as a champion of the project. We also developed a poster explaining indications for telemetry and problems with overuse and placed copies at medicine floor nursing stations. Data collection continued at 2 week intervals.
Results:
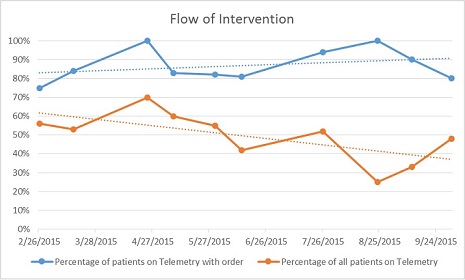
Baseline data in early 2015 covered 72 patients and showed that 39 (54%) were on telemetry and 8 (21%) did not have an order. After our educational interventions, another 60 patients were reviewed over two days in late 2015. Of these post intervention patients, 20 (33%) were on telemetry and 2 (10%) did not have an order.
Conclusions:
With simple educational interventions, we were able to reduce the use of telemetry without an order by 50% within six months. Telemetry cost is difficult to quantify but has been reported to cost at least $53 per patient per day. This equates to a $318 dollar savings between the two days measured in this study on a single unit in our hospital. If expanded throughout the hospital, this results in significant savings. In addition to an economic benefit, patients may enjoy a better experience with fewer tethers, unnecessary diagnostic tests, and interruptions as a result of false alarms, and staff may experience less alarm-fatigue.
Although our educational interventions have decreased the overutilization of telemetry, more interventions are necessary to achieve sustained change. Next-steps include changing the ordering system to require that an indication be specified before initiating monitoring and developing a nursing workgroup to address nursing overuse without an order. Although these interventions may ultimately be needed in order to reduce telemetry overutilization, the educational projects explored in this study form a framework for change by prompting staff to consider indications prior to initiating telemetry.