Background: Preventing readmissions of patients with chronic illness can improve healthcare outcomes and decrease costs. Previously reported Medicare claims data from 2003 to 2004 showed that 19.6% of Medicare beneficiaries discharged from the hospital were readmitted within 30 days at a cost of $17.4 billion. Our 232-bed community hospital has set a goal to reduce avoidable readmissions.
Purpose: The goal of the Transition of Care Clinic (TCC) is to provide timely and comprehensive outpatient follow up for patients discharged from an acute care hospital.
Description: The TCC is structured to provide interventions post hospital discharge which are focused on continued improvement and stability of health. The clinic is located in an ancillary service setting and can provide diagnostic and therapeutic interventions that are not usually available in primary care clinics. The clinical interdisciplinary team includes a hospitalist, a registered nurse, case management registered nurse, and a medical assistant. Using the LACE + Score, patients at high risk for readmission are identified and an ambulatory referral is placed to the TCC prior to discharge. The TCC post discharge care management process begins with a phone call to patients within 2 business days after discharge. At that time, a detailed questionnaire is utilized during a telephonic interview by the case manager that reviews the patient’s hospitalization, medications, transportation needs and schedules a timely appointment to the TCC. During the clinic visit, a comprehensive 30-day plan is developed with patient and family involvement. This includes education on medical disease states, changes in health, social status and prognosis. A thorough review and understanding of hospital findings and new medications has been found as keys in readmission prevention. Follow-up visits include additional TCC appointments and evaluation of home social service needs. Upon completion of the 30-day treatment plan, the patient’s care is transitioned to their primary care physician.
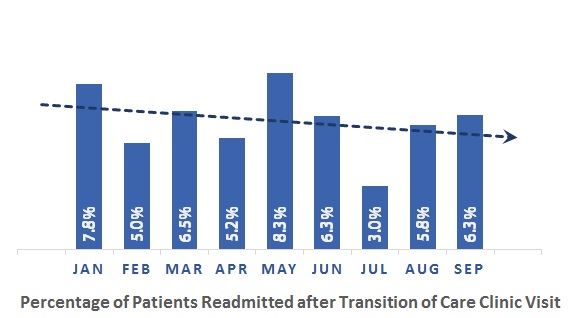
Conclusions: The TCC has had a direct impact in decreasing the hospital’s readmission rate. The baseline readmission rate for Medicare beneficiaries prior to the formation of the TCC was 15.44%. The 30-Day Hospital-wide All Cause Readmission Rate for year to date 2017 is 9.74% while the 30-Day All Cause Readmission Rate for patients that attended the TCC is significantly lower (see graph below). The TCC has proven to be an important part of the discharge process at our community hospital and resulted in a significant decrease in hospital readmissions.