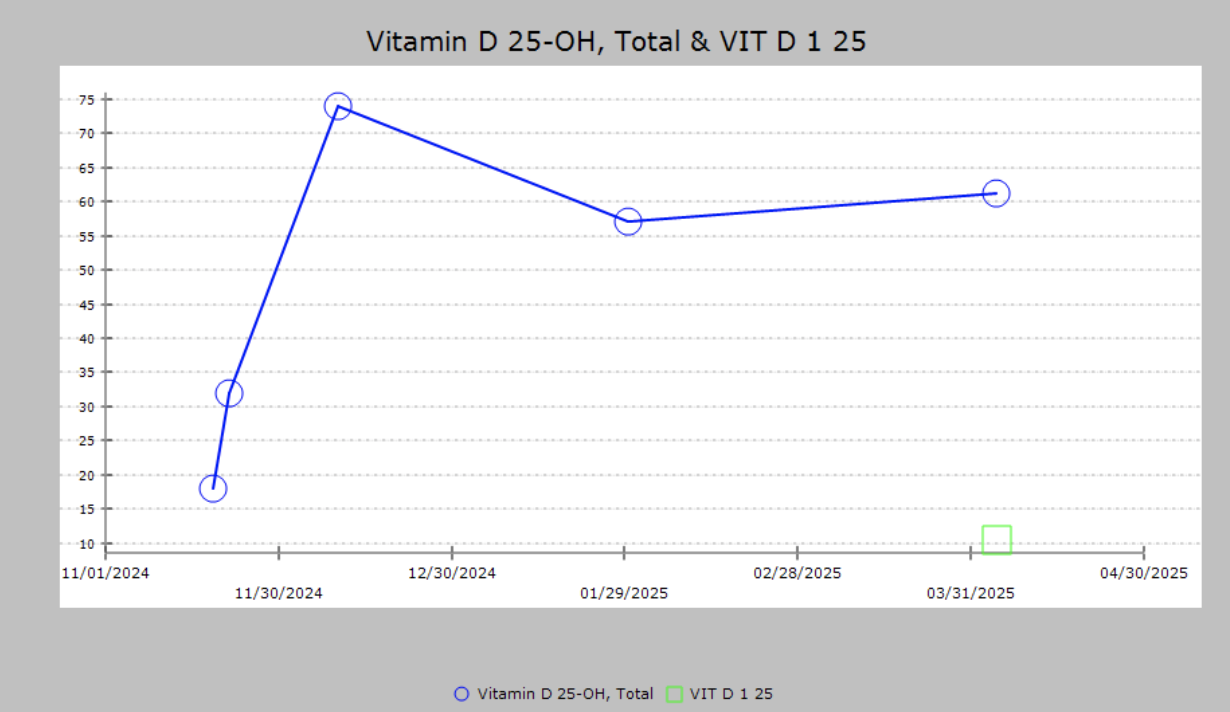
Case Presentation: A 34-year-old female with a history of focal epilepsy diagnosed during childhood complicated by status epilepticus, anxiety, depression, ADHD, and history of chronic hyponatremia presented to the hospital at 25 weeks gestation with complaints of recurrent seizures. During the admission process she had multiple witnessed generalized tonic-clonic seizures with nystagmus requiring multiple rounds of emergent intravenous medications including lorazepam, levetiracetam, and magnesium. Her symptoms soon progressed to refractory status epilepticus which triggered persistent fetal decelerations. The patient required emergent intubation and sedation and was brought for emergency caesarian section by the obstetric team. Laboratory investigations revealed profound hypocalcemia with a serum level of 5.3 mg/dL without significant renal or hepatic dysfunction. After delivery, the patient was transferred to the neurocritical care unit and reloaded with levetiracetam. She required trials of multiple antiepileptic infusions including fosphenytoin, phenobarbital, ketamine, and midazolam for seizure suppression until optimal control was achieved. Judicious monitoring and replacement of calcium was crucial throughout her hospital stay. Further evaluation revealed a 25-hydroxyvitamin D level of 18 ng/mL, suggesting significant hypocalcemia and vitamin D deficiency as the underlying etiology for the patient’s refractory status epilepticus. Upon discharge, she required an updated antiepileptic regimen as well as aggressive calcium and vitamin D supplementation.
Discussion: This patient’s history and medication review revealed chronic use of multiple anti-epileptic drugs, including phenytoin, phenobarbital, and carbamazepine. These agents, known as enzyme-inducing antiepileptic drugs (EIAEDs), are cytochrome P450 inducers and are associated with increased catabolism of vitamin D, thereby reducing calcium absorption and contributing to refractory hypocalcemia. Vitamin D plays a vital role in calcium homeostasis by promoting the expression of calcium binding proteins and transporters in the intestinal epithelium to enhance calcium uptake from the gastrointestinal tract. In deficiency states, intestinal calcium absorption may drop significantly, often resulting in hypocalcemia. Symptoms of neuromuscular dysfunction can occur such as muscle cramps, tetany, spasms, numbness or tingling in the fingers and around the mouth, fatigue, irritability, and in severe cases, seizures or cardiac arrhythmias. In this case, persistent hypocalcemia lowered the patient’s seizure threshold, culminating in super-refractory focal status epilepticus. A multidisciplinary approach was essential in managing this complex medical case. The admitting hospitalist was responsible for facilitating essential medical care between specialists including obstetrics, neurology, and endocrinology. An accurate history taking, extensive medication review, and broad differential diagnosis were instrumental in piecing together the sequence of events that lead to this patient’s extreme clinical presentation.
Conclusions: This case underscores the need for clinicians to maintain a high index of suspicion for metabolic disturbances in patients with refractory seizures, particularly those on long-term EIAED therapy. Regular monitoring of vitamin D and calcium levels should be considered in this population to prevent complications.
.png)