Case Presentation: A 66-year-old woman with hypertension presented to the hospital one day after arrival to New York City from Guinea with chronic daily vomiting, unintentional weight loss, progressive shoulder pain, and a subacute pruritic rash. She denied fevers, night sweats, difficulty breathing, chest pain, palpitations, unusual skin exposures, insect bites, trauma to the shoulder, and a history of joint problems. On exam, patient was hypertensive with otherwise stable vital signs, as well as with scaling plaques over legs and trunk, limited range of motion in her right shoulder, and asterixis. Labs were notable for a creatinine of 15mg/DL, nephrotic-range proteinuria, and normocytic anemia. Calcium was normal. The patient was admitted to hospital for acute renal failure and further workup.
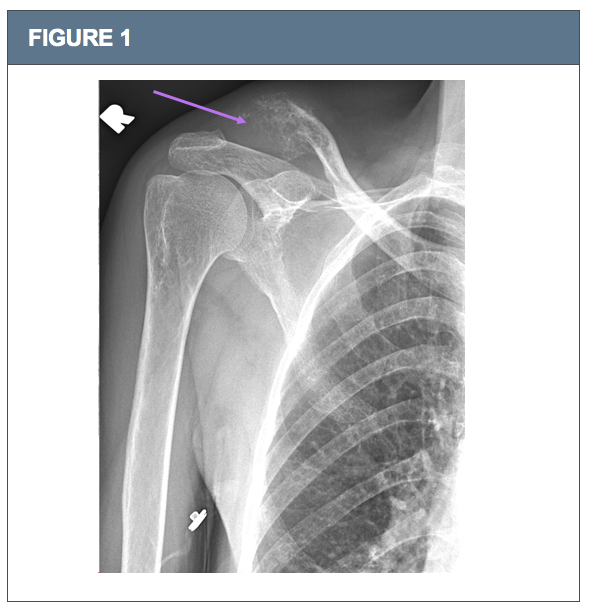
Discussion: This case highlights the diagnostic reasoning principles of Occam’s razor, Hickam’s Dictum, and Crabtree’s Bludgeon. Occam believed the diagnosis that most simply explains a case is likely to be correct. Hickam suggests that two or more horses are more likely than one zebra. Crabtree refers to an attempt to make data “fit” an explanation, ignoring inconsistencies that may suggest an alternative answer. Our own workup proceeded with the expectation of a unifying diagnosis to explain the wide constellation of presenting symptoms: renal failure, nephrotic-range proteinuria, rash, and shoulder pain.Shoulder x-ray showed osseous resorption of the lateral right clavicle with possible osteoid matrix deposition. Subsequent MRI suggested aggressive neoplasm. Primary Clavicular tumors are rare but can be seen with lytic lesions in older adults from multiple myeloma. Multiple myeloma could also account for renal failure, nephrotic-range proteinuria, and rash (thought secondary to uremia).But a longer-standing renal process was suggested by an atrophic left kidney on CT abdomen. CT chest showed bilateral lower lobe pulmonary nodules and nodular thyroid. Calcium, SPEP/UPEP, and kappa/lambda ratio were all normal, and a skin biopsy suggested paraneoplastic dermatitis – all data inconsistent with multiple myeloma. To our surprise, shoulder biopsy revealed metastatic follicular thyroid carcinoma. Two processes were at play: the first, end stage renal failure. The second, a common malignancy with uncommon metastasis.Following a diagnostic error, the Clinical Excellence Commission suggests conducting a “cognitive autopsy” on a case, including consideration of preceding events and how cognitive biases, ambient conditions, and emotions contributed. Thyroid malignancies most commonly metastasize to lung, then bone, though report of clavicular involvement is sparse in the literature. In haste to find a unifying diagnosis, we focused less on silent data, like the pulmonary nodules thought incidental – considering these as potential metastases may have helped broaden our differential.
Conclusions: Perhaps an absence of regular healthcare decreases Occam’s positive predictive value. The final diagnoses were primary end stage renal disease of unknown etiology (biopsy-deferred), and follicular thyroid carcinoma with metastases to the clavicle and lungs with paraneoplastic rash. Clinicians should go through a cognitive checklist not only after an error, but also in the midst of a case with many moving parts and no clear answer. These diagnosis aids should remind us of several principles: take a step away; consider emotions, conditions, biases; engage Type 2 thinking; acknowledge Occam, Hickam, and Crabtree.