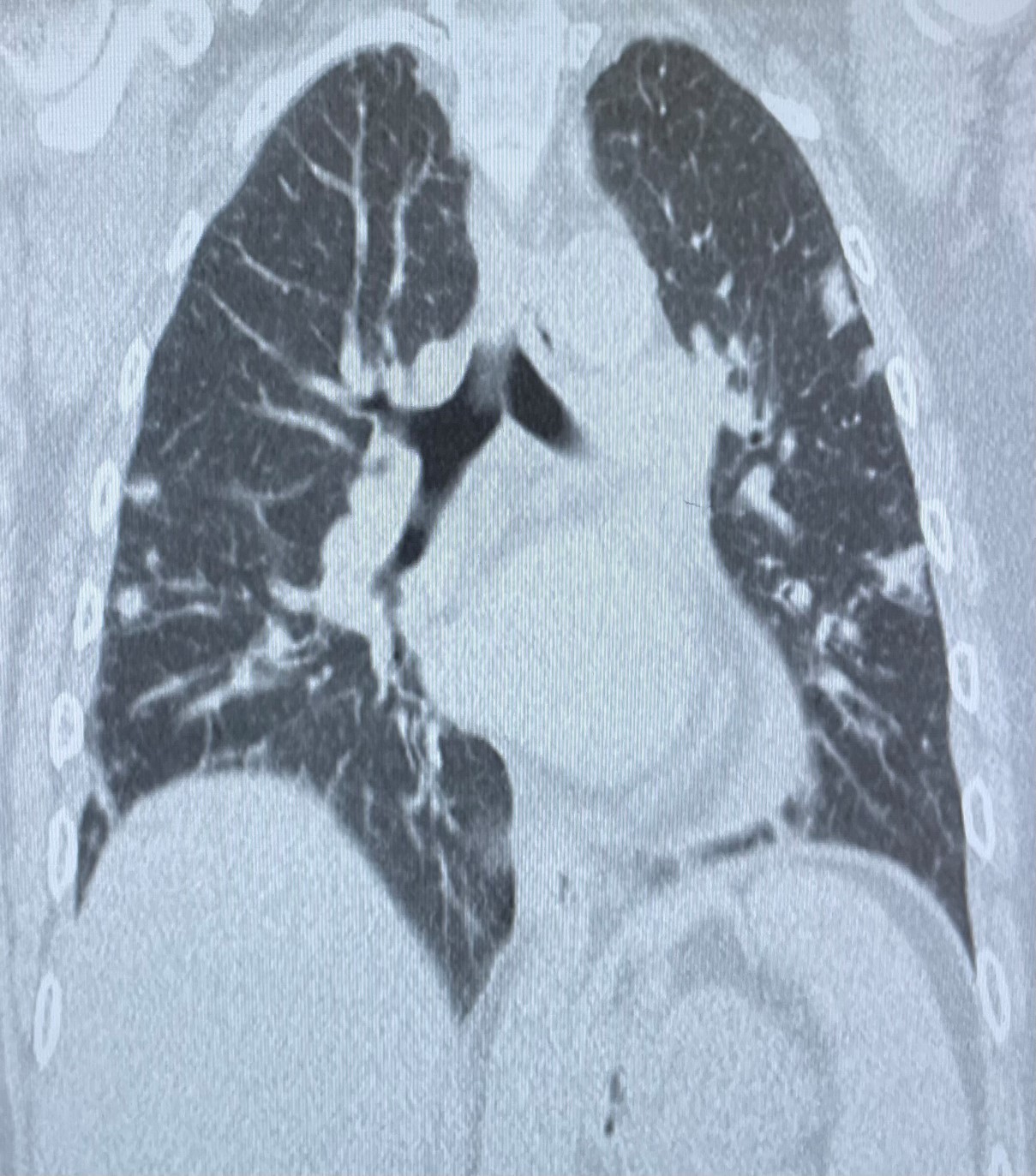
Case Presentation: A 58-year-old woman arrived to the emergency room complaining of fevers, chills, and confusion for two weeks. She has hypertension, complex psychiatric conditions including anxiety, depression, and alcohol use disorder. Her symptoms began 14 days ago with non-productive cough and headaches. During this time she also experienced fevers and chills. On physical examination, the patient seemed alert but lethargic. Her Cardiovascular examination revealed a normal heart rate, regular rhythm, and no murmurs. Respiratory examination showed clear breath sounds on both sides without wheezing. Abdominal examination was benign, no tenderness was appreciated.She was vitally stable on presentation . Labs showed elevated white count and inflammatory markers with Procalcitonin at 4.35 ng/ml, CRP at >300 mg/L. Rest of the labs showed a normal troponin level and initial EKG was insignificant with very minimal ST depression.She was given broad-spectrum empiric antibiotic coverage. CT scan of the chest revealed bilateral nodules with indistinct boundaries and cavitation dominant in the upper lobe and periphery, findings congruent with disseminated septic emboli. Two blood cultures drawn from separate sites were positive for Streptococcus anginosus, a sub-group of viridans Streptococci. To investigate further, TTE was done which was unremarkable. This was followed by TEE which was negative for any vegetation, but was significant for Chiari network within the right atrium.
Discussion: While Chiari networks may not typically lead to symptoms or complications, the situation with our patient differed, as it presented with severe sepsis. Therefore, a decision was made to treat it as a case of infective endocarditis due to the potential for contributing to embolic events and increasing the risk of infectious complications. The patient was released with a prescription of ceftriaxone 2g intravenously daily to complete 6-week treatment. Patient was advised to schedule a follow-up appointment with the pulmonology clinic in 4-6 weeks for a repeat CT chest scan to monitor the resolution of nodules.In the above case, the patient fit Duke’s criteria for possible IE due to the presence of two separate blood cultures growing viridans Streptococci, and the presence of septic emboli to both lungs on CT scan of her chest. Despite negative findings on the TTE and TEE, the patient was treated with an antibiotic regimen tailored toward IE. It is likely that the presence of the Chiari network in her heart, combined with existing risk factors in her case of chronic alcoholism and frequent dental procedures resulted in an infection around the network in RA resulting in IE.
Conclusions: Infectious complications occurring due to right atrial embryonic remnants (RAER), such as Chiari network, Thebesian valve, Eustachian valve, etc. are often underreported and underestimated (9). Cresti et al., found the frequency of RAER endocarditis to be 16% among right-sided IE cases, and 2.5% of complete IE cases. Due to their appearance on echocardiograms, they can often be missed completely (10).It is possible that minor vegetations were present on the network but had either disseminated or were too small to identify. Due to their varying size and complicated structures, right atrial embryonic remnants are known to be notorious in escaping imaging, and make visualization of infective vegetation challenging. European Society of Cardiology recommend treating them like IE despite absence of characteristic imaging (11).