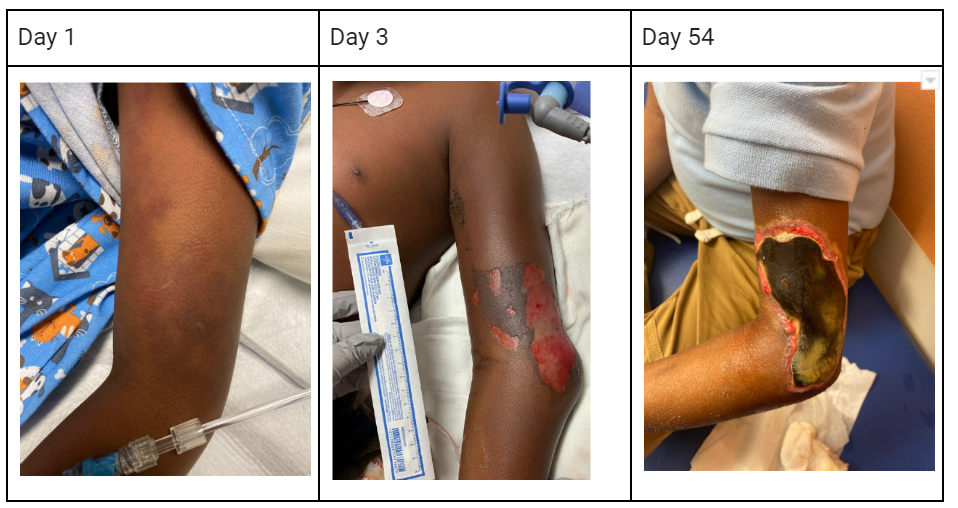
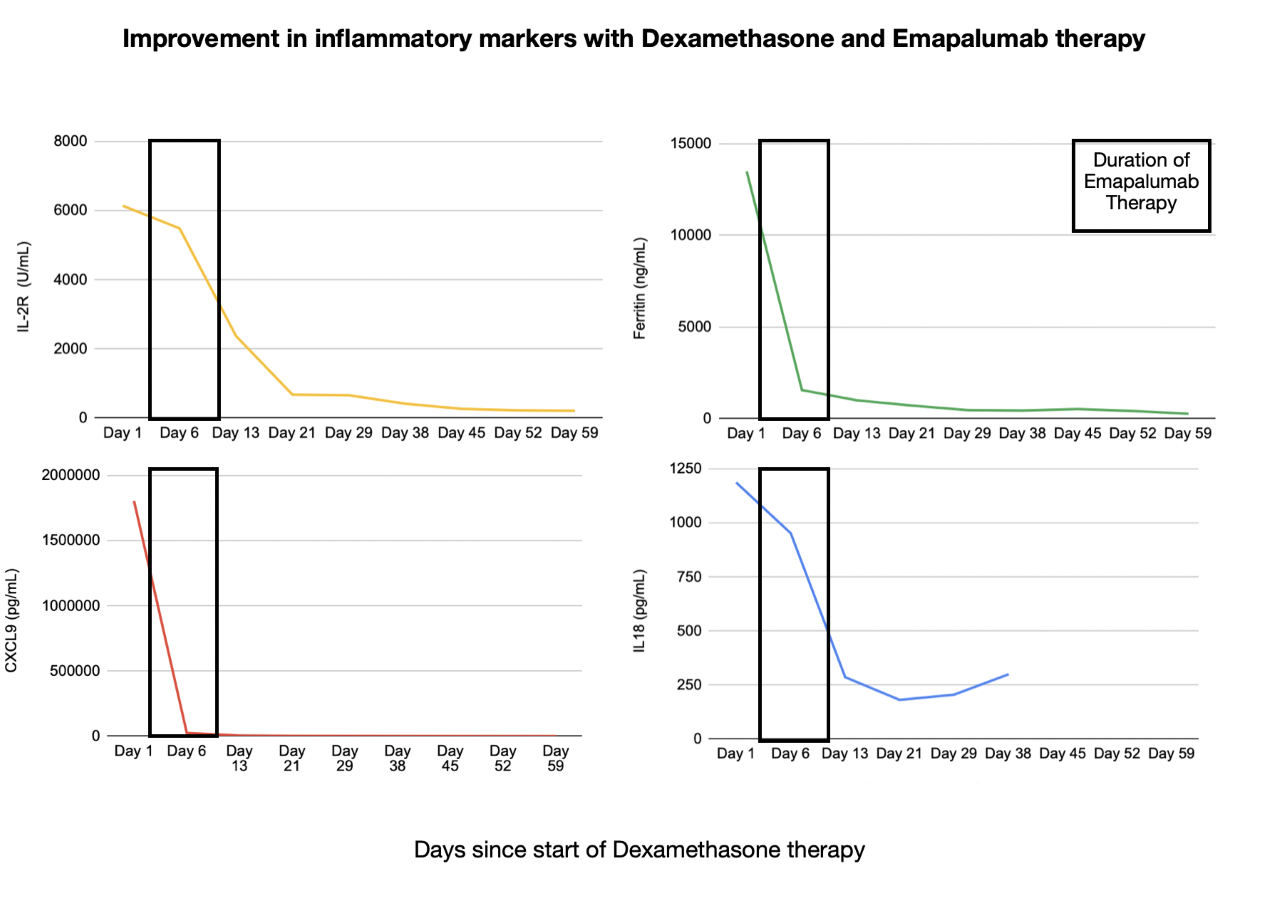
Case Presentation: Although infrequent, systemic loxoscelism can occur following a brown recluse spider bite and result in dermal necrosis, hemolytic anemia, DIC and renal failure. We present a case of an eight year old male who developed Hemophagocytic Lympho-Histiocytosis (HLH) secondary to systemic loxoscelism. The patient presented with gross hematuria, abdominal pain, and fever. The physical exam showed a single vesicle on the left upper extremity surrounded by ecchymosis with erythematous streaks (figure 1). Initial labs showed hemolytic anemia, hematuria, Stage 3 AKI, severe Anion gap metabolic acidosis, transaminitis, hyperbilirubinemia and elevated inflammatory markers. Patient was noted to be encephalopathic on presentation. EEG showed slowing of background waves, but no seizure activity. Electrolyte abnormalities and AKI were addressed by Continuous Renal Replacement Therapy. Hypertension (At presentation 140-142/90-99), was addressed with medication. Due to fever, elevated inflammatory markers, and multi organ dysfunction with ongoing encephalopathy, ferritin levels were obtained and were elevated to 10,858 ng/mL (10-140 ng/ml). This prompted further workup for HLH. Bone marrow aspirate was consistent with HLH. CXCL-9, IL-2R and IL 18 were significantly elevated (figure 2). Dexamethasone and Emapalumab initiated, which led to resolution of symptoms and improvement of multi organ dysfunction including encephalopathy.
Discussion: The HLH-2004 trial established the diagnostic criteria (1). According to this criteria patients must either have a family history or molecular diagnosis consistent with HLH. If that is negative or unavailable then patients must have five of eight findings: fever, splenomegaly, bicytopenia, hypertriglyceridemia and/or hypofibrinogenemia, hemophagocytosis, low/absent NK-cell-activity, hyperferritinemia, and high-soluble interleukin-2-receptor levels (1). Our patient met 6 of the 8 criteria. Loxoscelism is a very rare cause of HLH with only three cases reported in the literature. HLH workup in these cases was pursued due severe multi organ failure, lack of clinical improvement or decrease in inflammatory markers despite antibiotics. Initiation of Dexamethasone led to resolution of symptoms (3-5). This is the first reported case of encephalopathy as one of the presenting symptoms of HLH secondary to systemic loxoscelism. Literature review of systemic loxoscelism without HLH was notable for a few cases with encephalopathy however the underlying etiology included PRES, substance withdrawal and high dose steroid use(6). Dexamethasone is the cornerstone of HLH therapy however, due to the severity of presentation and elevation of lab markers, glucocorticoid therapy was supplemented with Emapalumab. Emapalumab is a newer monoclonal antibody approved for treatment of primary HLH with refractory, recurrent, or progressive disease or intolerance to HLH therapy (6). Emapalumab is still being investigated for treatment of secondary HLH but has been shown to be effective in animal studies (6).
Conclusions: Envenomation with a brown recluse bite in can lead to systemic loxoscelism. HLH is an extremely rare complication of systemic loxoscelism. Patients presenting with fever and elevated inflammatory markers as well as severe organ dysfunction, in particular encephalopathy, should be investigated for underlying HLH. Ferritin can be used as an initial screening tool, if elevated, should prompt further evaluation of HLH markers.