Background: Despite the efforts of medical professionals to gain a comprehensive understanding of the individuals and the population they serve; it is often difficult to get to know the intimate details of a patient’s socioeconomic background. This can result in a gap between the care plan prescribed by physicians, and the capacity of the patient to complete that plan. An example is clearly seen in a study done by Cornelius et al. In this study, the lack of basic access to social support and services correlated with lower treatment self-efficacy. Transportation was significantly directly related to decreased adherence (Cornelius, 2007). While there are community resources (public transport, soup kitchens) that can potentially alleviate this need, there is little understanding of the prevalence and the proficiency of these organizations to provide realistic support. There seems to be a gap between the available resources and usage of them. We believe that that social determinants contribute to this. Screening for socialdeterminants of health is now a requirement of all government payor contracts. NHRMC is embarking on how best to screen and how to meet the needs of our patients.
Methods: As part of a quality improvement project, Internal Medicine House Staff initiated SDOH screening in our inpatient patient population. 100 patients were interviewed face to face by a member of the health care team in regards to availability and reliability of transport in their area, their financial ability to provide food for the household, and the overall ability for the household to provide for the basic necessities. SDOH needs were trended as well as narrative data given by patients.
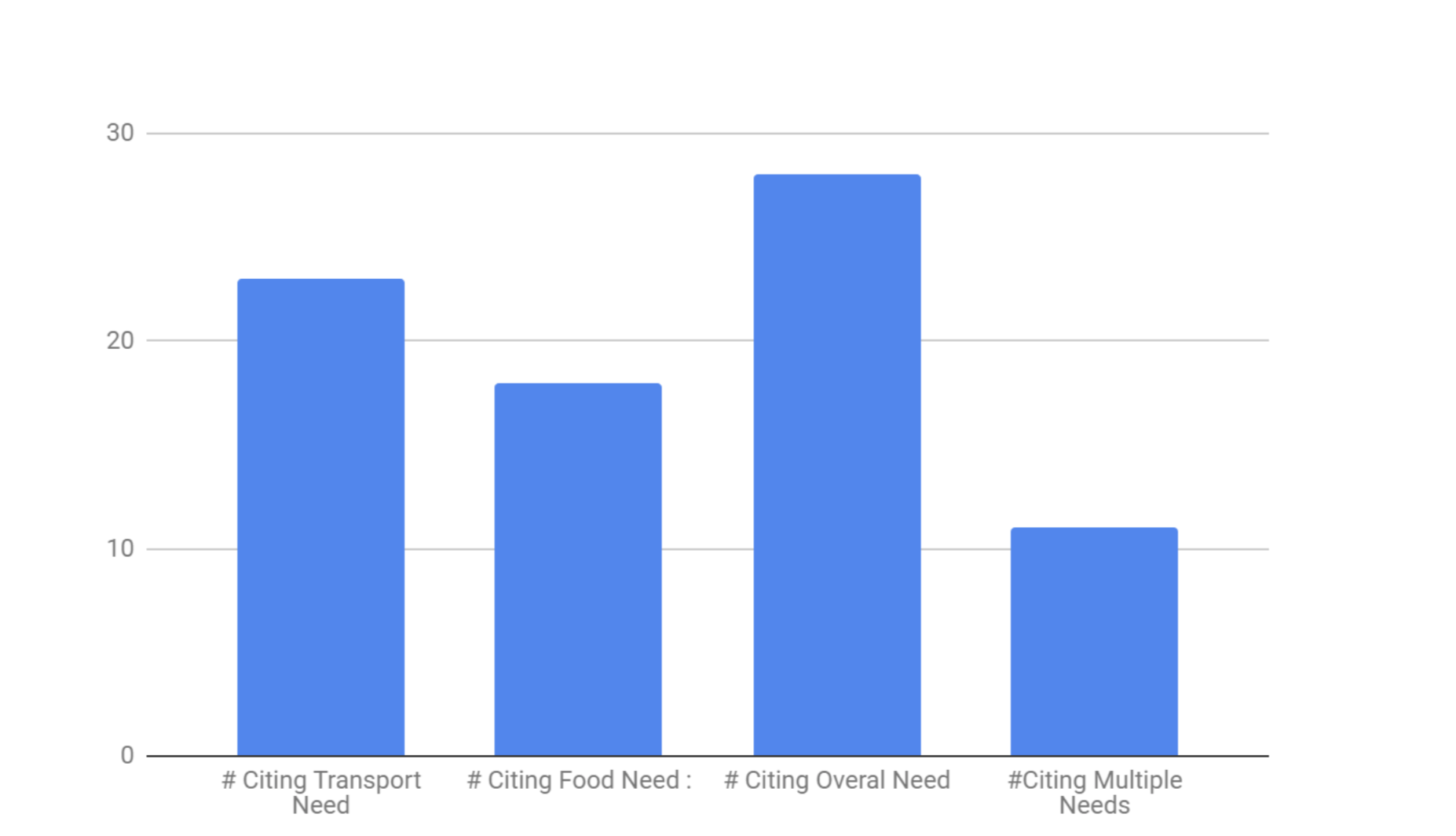
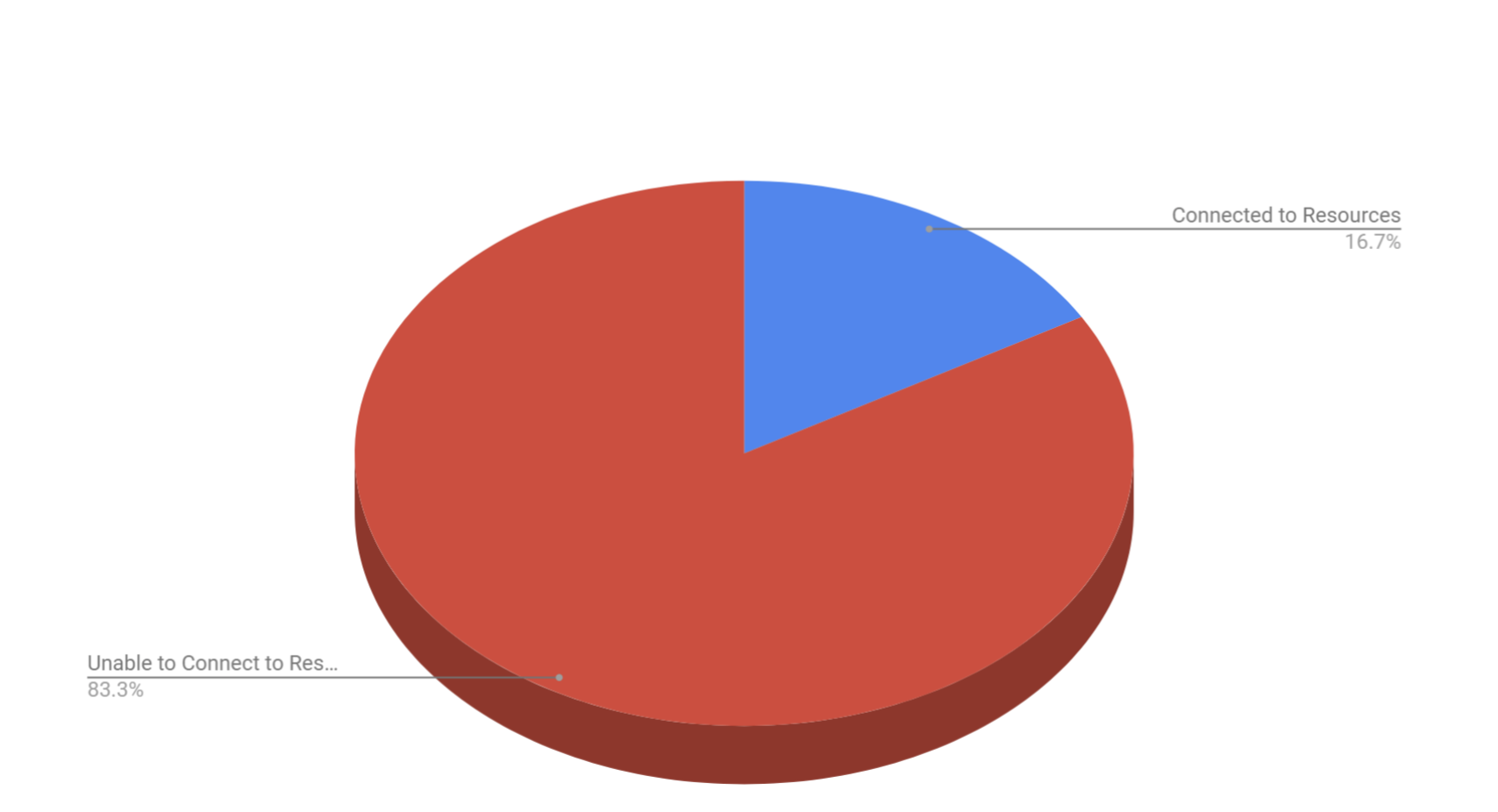
Results: The interviews revealed that 39.2% of patients faced a need that had a direct impact on their health, and only 16.7% of those patients faced barriers that community based organizations were potentially able to combat. Those barriers can be further broken down into transportation, food, and financial resource strain. Transportation as a need was cited 63.8% of patients and food was cited 50% of the time. The primary need faced by the community at large was a non-specific financial need, affecting 77.8% of patients in need. Since the barrier was financial and there was no specific cause, there existed little to no support organizations in the area.
Conclusions: As physicians gain a greater understanding of the socioeconomic barriers their patients face, there is a possibility for further individualization of post-hospital prescribed action. The percentage of transportation , food, and financial needs were a significant portion of those citing needs. As evidenced by Marmot et. al upstream social factors , while poorly understood, significantly impact the health of patient. No longer can the impact of social determinants be ignored (Braveman, 2014). There is a clear need for further research. Firstly to further characterize the issue and secondly to begin understanding a sustainable solution.