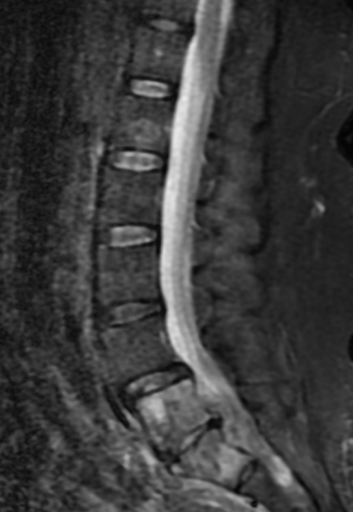
Case Presentation: A 56-year-old female with a history of cervical cancer in remission, post-chemotherapy and total hysterectomy, and insulin-dependent diabetes mellitus, was admitted for worsening chronic lower back pain, which had intensified over the past two weeks. She denied paresthesia or weakness. On examination, she was diaphoretic, shivering, and afebrile, with a blood pressure of 159/112 mmHg and a heart rate of 154 beats/minute. There was diffuse tenderness in the lower back, but no neurological deficits. Initial labs showed leukocytosis (20,450/mm³ with a left shift), lactic acid of 3.1 mmol/L, bicarbonate 10mmol/L, glucose of 456 mg/dL, and ketonuria, suggesting diabetic ketoacidosis. Blood and urine cultures were obtained, and broad-spectrum antibiotics (Cefepime and vancomycin) were initiated for suspected pyelonephritis. The patient was admitted to the ICU for diabetic ketoacidosis management.A CT of the abdomen and pelvis with contrast revealed right-sided hydroureteronephrosis, without calculi, and a nephrostomy tube was placed. As her back pain persisted with a new onset of muscle cramps in her lower extremities an MRI of the thoracic and lumbar spine was ordered that revealed osteomyelitis, discitis at the L5-S1 level, and an anterior epidural abscess (2.3 x 0.9 cm), causing canal stenosis. She was transferred to a neuro-ICU for neurosurgical evaluation. Cultures from the urine grew Klebsiella pneumoniae and Escherichia coli, and blood cultures identified Streptococcus constellatus. Based on sensitivity results, antibiotics were narrowed to Ceftriaxone.The neurosurgeon recommended non-surgical management, as the patient’s back pain improved, and her neurological exam remained normal. Further investigations, including Maxillofacial CT and Transesophageal Echocardiogram, revealed no abscess or vegetation, respectively. A bone biopsy confirmed acute osteomyelitis, but no malignancy. Cultures from the biopsy and repeat blood cultures showed no growth, and inflammatory markers (ESR, CRP) downtrended. The patient was discharged on IV Ceftriaxone (2 grams daily) to complete a seven-week course.
Discussion: Spinal Epidural Abscess (SEA) is a rare but potentially life-threatening condition, with an incidence of 0.2 to 1.2 cases per 10,000 hospital admissions. The routes of infection include hematogenous spread, contiguous infection from nearby structures, or following invasive procedures. SEA can lead to paralysis or death if not diagnosed and treated promptly. While standard treatment involves decompressive surgery and drainage, neurologically stable patients can be managed conservatively with prolonged IV antibiotics. In this case, despite the lack of a clear infectious source, the patient was successfully managed with antibiotics after her neurological exam remained stable and no further surgical intervention was needed.
Conclusions: This report presents a rare case of spontaneous epidural abscess with no neurological deficit and pyelonephritis. The infection occurred without an identifiable source, and cultures revealed different bacterial species in the blood and urine, complicating the diagnosis. The presence of two primary infections—epidural abscess and pyelonephritis—made diagnosis challenging. This case highlights the importance of maintaining a broad differential diagnosis in patients with nonspecific back pain, particularly those with uncontrolled diabetes and cancer, and the need for early prolonged antibiotic (6-7 weeks) treatment.