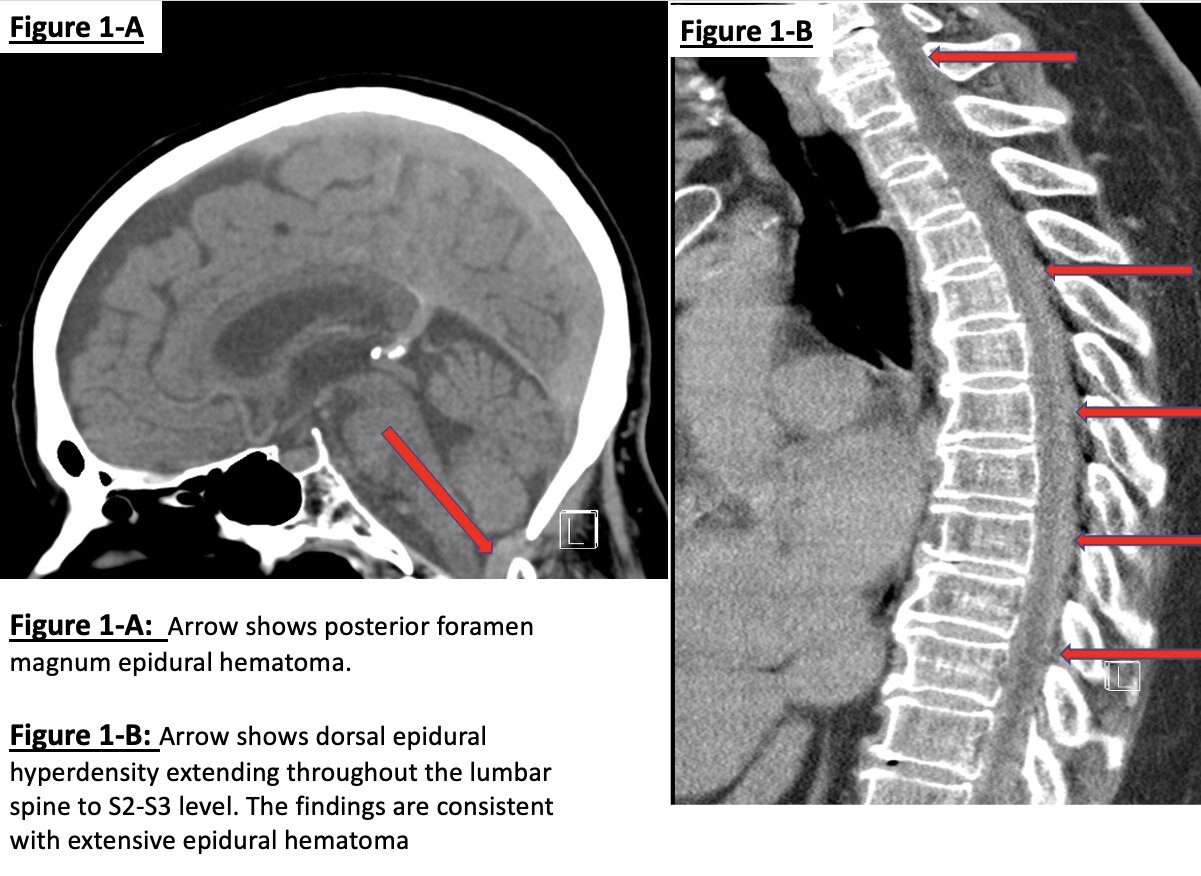
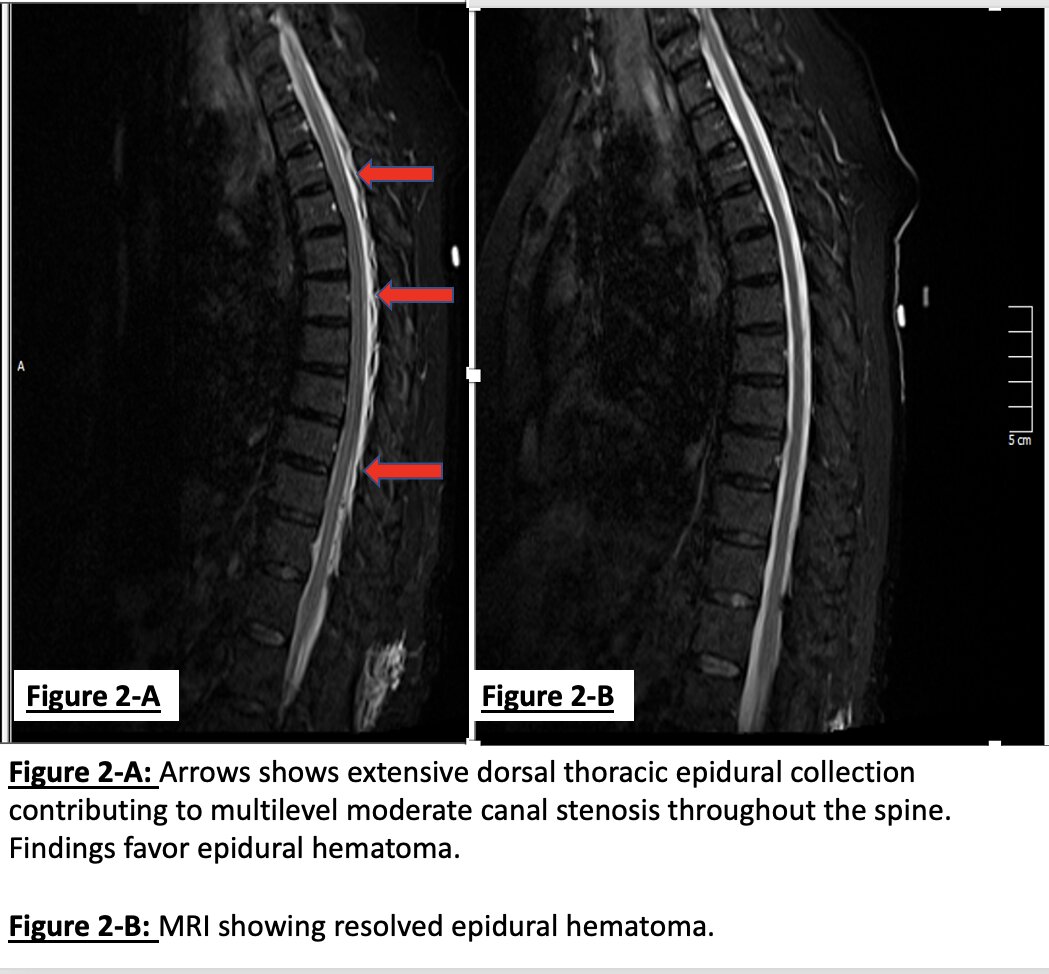
Case Presentation: Spontaneous spinal epidural hematoma (SSEH) is a hematoma that happens without an insult. Although a rare entity, it can result in spinal cord compression. Etiologies include anticoagulant therapies, coagulopathies, blood dyscrasias, pregnancy, and vascular malformations (1). We present a case of SSEH in the setting of heparin and clopidogrel use during a vascular procedure. A 72-year-old female with a history of coronary, peripheral vascular disease, and stroke 20 years ago was brought in with severe neck pain and an inability to move any of the extremities after an outpatient femoral-popliteal bypass by vascular surgery. Heparin 6000 units were administered intravenously during the procedure. The neurological physical examination revealed no tone, power, or sensation in the upper extremities, whereas the lower extremities showed no sensation, no tone, and a power of 1/5 on the left and 0/5 on the right extremity. She also experienced sudden onset hypoxia and required intubation in the emergency department. Clopidogrel, one of her home medications, was last taken 24 hours ago. Blood work showed an elevated partial thromboplastin time of >100 seconds (normal: 26.2-38.8 seconds), with the rest of the laboratory values being unremarkable. The CT scan of the head, lumbar, and thoracic spine showed an extensive spinal epidural hematoma, as shown in figures 1-A and 1-B. The MRI also showed extensive epidural hematoma, as shown in figure 2-A. Due to possible heparin toxicity, she was given protamine sulfate and desmopressin. After being transferred to the medical intensive care unit (MICU), the neurological examination of the patient improved dramatically in a short time, and she was extubated. The follow-up MRI shown in figure 2-B showed almost complete resolution of the SSEH.
Discussion: Heparin can result in bleeding as a complication in 3-33% of patients with or without thrombocytopenia (2). Clopidogrel may have some benefits in preventing ischemic stroke and myocardial infarction, but the reported bleeding rate is 1.4% (3). To our knowledge, the literature review has shown six cases of clopidogrel-induced SSEH (4) and only four cases of enoxaparin-induced SSEH (5), with one case of spinal anesthesia-induced spinal epidural hematoma in a patient treated with both clopidogrel and enoxaparin (6). Another case of SSEH was reported after heparin usage, with a history of epidural tumor (7). Overall, the literature fails to impart SSEM solely after heparin usage unless a preceding spinal tap is executed (3). Our case is unique as the patient was on clopidogrel and received heparin during femoral popliteal bypass surgery. The mainstay of the treatment is urgent surgical evacuation and decompression (1). However, a few cases of SSEH do resolve on their own. Conservative management should be used only on patients who are rapidly improving neurologically (3).Our patient had quick neurological improvement, and her symptoms resolved spontaneously on their own after the reversal of heparin toxicity.
Conclusions: In conclusion, we believe that SSEH was related to heparin use and was exacerbated by clopidogrel. Antiplatelet drugs can cause this rare complication, which is a neurosurgical emergency. Physicians should be aware of it so that a timely intervention can be done if necessary, especially in the era of excessive anti-platelet prescriptions.