Background: Our 165-bed community hospital is in a phase of rapid growth due to demographic changes and expansion of services offered within the hospital. While offering unprecedented level of healthcare access to the community, improvement with emergency department (ED) throughput has emerged as one of our challenges from a patient safety perspective. Unnecessarily prolonged ED wait times have been associated with decreased patient and ED staff satisfaction, and higher cost of care.
Purpose: We structured an initiative to streamline the admission process around the Plan-Do-Study-Act ( PDSA ) model to identify bottlenecks impacting in-patient transition of care; to implement a proactive initiative addressing the barriers; and to evaluate this initiative’s impact on ED to in-patient transition time and make further practice changes as appropriate.
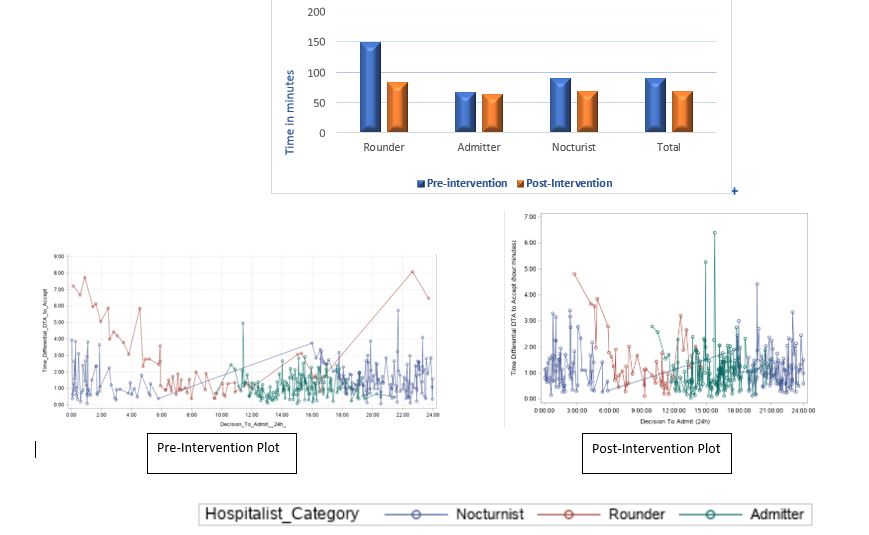
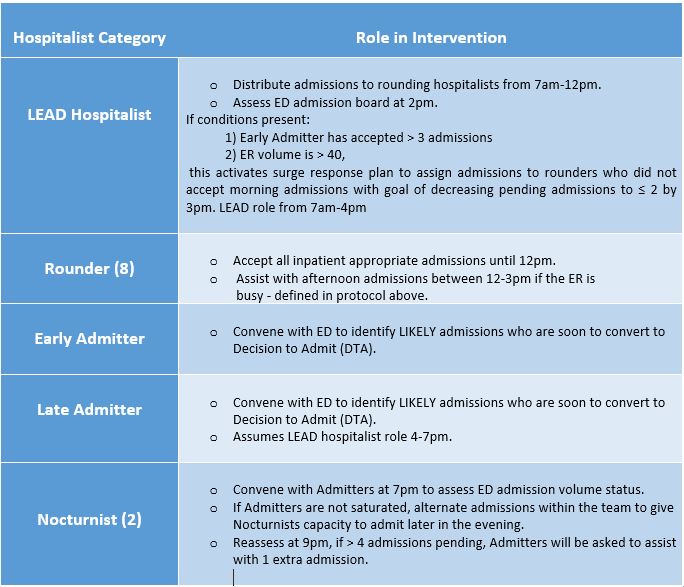
Description: A focus group comprised of volunteer hospitalists was tasked with this initiative. Admission data was collected retrospectively for 15 consecutive days in August 2019. Time specific data for each admission was obtained, including Decision to Admit time (DTA), hospitalist Accept Time (AT), and admitting hospitalist category. The initial plot (Table 1) shows a surge of admissions between midnight and 2 am with a few patients not being evaluated overnight (1.9/night). Consequently, delayed admissions pending for day team hospitalists, resulted in prolonged ED length of stay. Using computerized hospital-ED tracking system we formulated a trigger-response protocol to predict volume of admissions, allowing us to respond proactively to any surges (Table 2). Post-intervention, data was collected for 14 consecutive days in October 2019 and measured variables were compared (Table 1).Results: A total of 802 admissions were assessed; 409 (29.2/day) pre-intervention and 393 (28.1/day) post-intervention. Data was analyzed using SAS 9.3. DTA to AT was used as a surrogate marker of avoidable ED wait time. There was a statistically significant improvement in DTA to AT by 20.4 minutes [95% CI 18.6-22.3 minutes, p<0.01 (paired t-test)] from 91 minutes to 69 minutes, a 22% improvement. This translates to 9.5 patient hours per day reduced in ED throughput time. A significant reduction in number of delayed overnight admissions was observed, decreasing from 30 to 14 patients pending admission in the morning, pre and post intervention, respectively; a 53% reduction.
Conclusions: Through this quality improvement initiative, our team was able to improve ED wait times. Further, our model has the potential to serve as a replicable template to explore more concrete outcomes including patient and staff satisfaction, and cost and quality of patient care.