Background: Rising inpatient complexity, residency duty-hour reforms, and anticipated national physician shortages are placing increasing strain on the hospital medicine workforce, resulting in greater utilization of nurse practitioners (NPs) and physician assistants (PAs). Despite this growing reliance on NP/ PA hospitalists, reports describe a wide variation in hospital medicine (HM) onboarding, limited pre-licensure HM-specific training, and few structured NP/PA HM fellowships.
Purpose: To evaluate a standardized 12-month hospital medicine transition-to-practice (TTP) program for NPs and PAs using prospectively collected program evaluation data, focusing on knowledge, confidence, satisfaction, and the relationship between live versus asynchronous participation and outcomes.
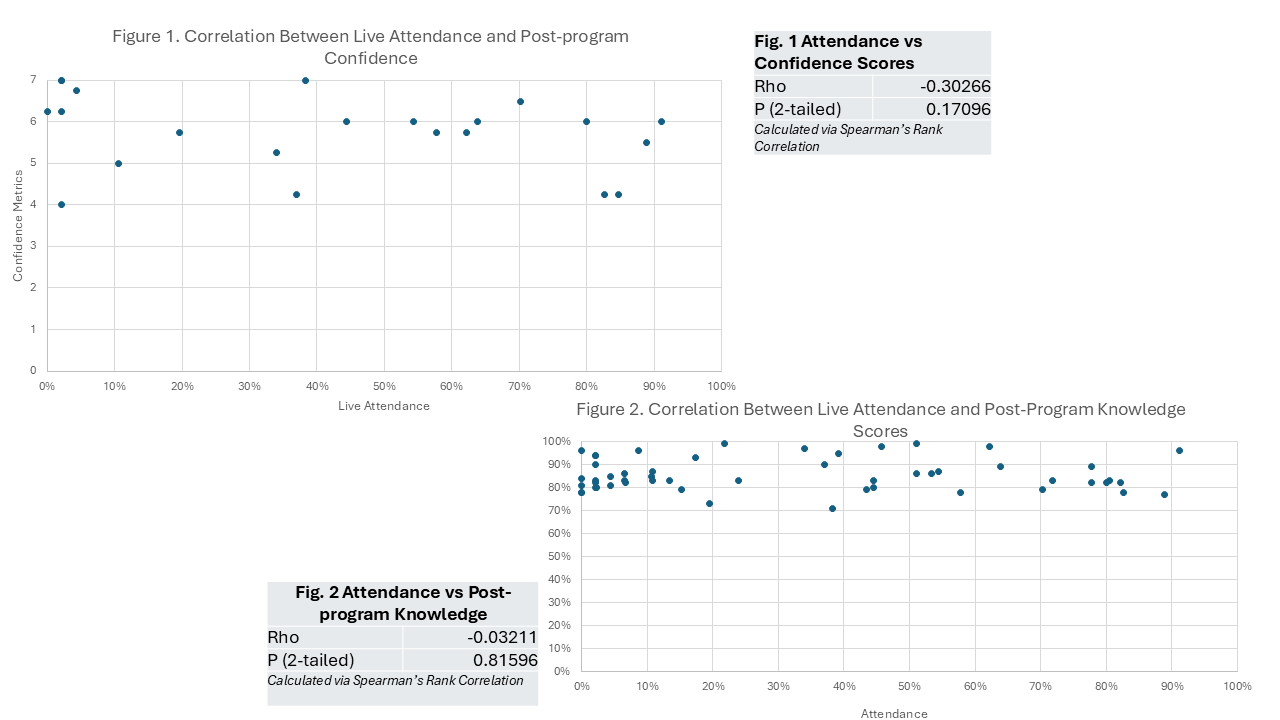
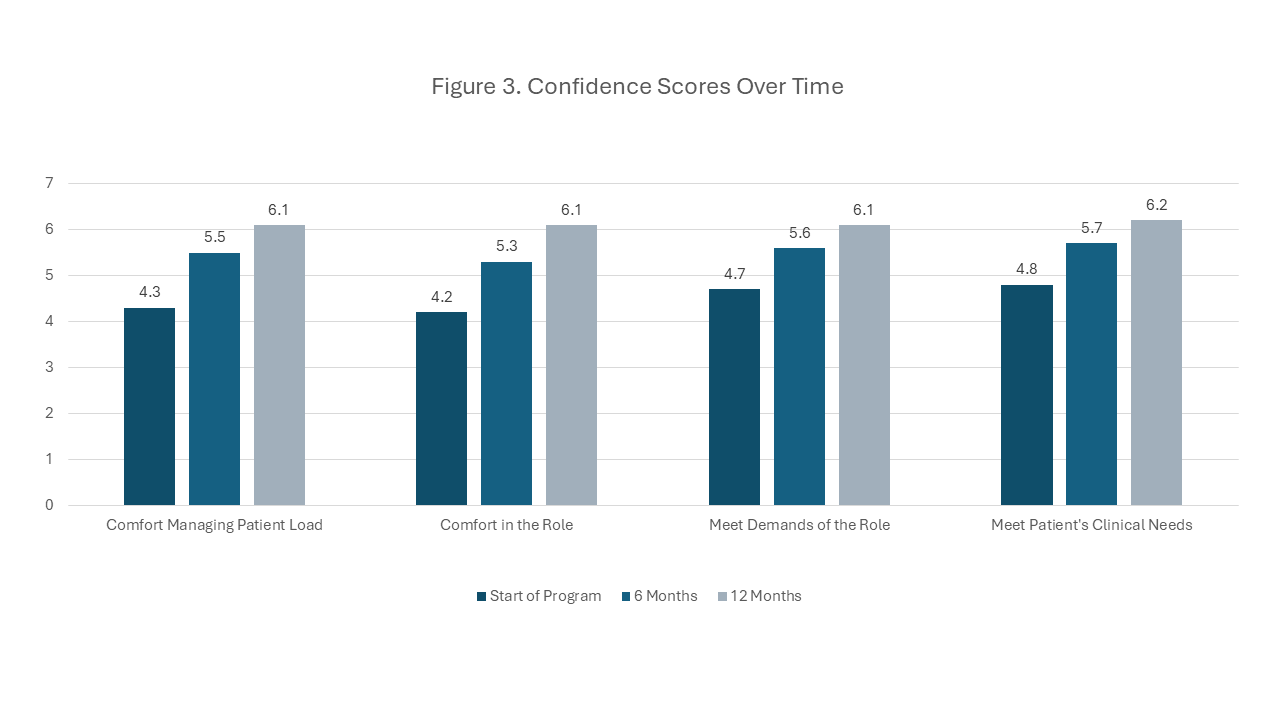
Description: A standardized 12-month HM TTP program was developed using ABIM and SHM frameworks. Content was delivered both live and asynchronously to accommodate varied schedules. Each weekly 90-minute session integrated didactics, case-based learning, professional development, and structured guided readings. Evaluation followed Kirkpatrick’s model: Level 1 (reaction) via weekly satisfaction ratings and exit surveys; Level 2 (learning) via pre- and post-program knowledge tests and confidence assessments at baseline, mid-program, and completion. Knowledge assessments used National Board of Medical Examiners (NBME)-style multiple-choice questions aligned with the weekly learning objectives. Confidence across 4 domains was measured on a 7-point Likert scale. Quantitative data were analyzed descriptively and with Spearman’s rank correlation and paired T-test. Since 2022, 144 clinicians (50 PAs, 94 NPs) have participated in the program, with 78 active participants and 66 graduates. At enrollment, 54.8% reported fewer than two years of experience. The cohort represented 31 medical centers across 18 states.Average satisfaction with program lectures was 4.7/5. Presentations in the Foundations block scored lowest (4.35/5), with the highest scores in neurology and cardiovascular (4.76/5). Mean pre-post knowledge scores increased by 11% (range 1–32%, p< 0.001, paired t-test). Self-reported confidence improved significantly in all domains (p< 0.001, paired t-test), with the largest numerical increase in “comfort in the role” (mean of 4.2 to 6.1). Most (74%) attended live < 50% of the time, and 25% relied solely on asynchronous recordings. No significant correlation was detected between live attendance with knowledge acquisition (ρ= -0.03, p = 0.81, Spearman’s) or post-program confidence (ρ= -0.3, p = 0.17, Spearman’s).
Conclusions: This TTP program addressed the educational needs of a heterogeneous cohort of new and experienced APPs entering hospital medicine by providing HM-specific, clinically relevant training. Participants reported high satisfaction with the program webinars. Statistically significant improvements in knowledge and confidence were observed on program assessments, supporting objective and subjective learning gains. Gains were independent of live attendance, underscoring the value of asynchronous access for those with variable schedules. Limitations include a lack of a control group and potential selection bias, limiting generalizability. Ongoing curriculum refinement and longitudinal data collection through year five are planned.