Background: In surgical co-management (SCM), surgeons and hospitalists share responsibility of care of the surgical patients. In August 2012, we implemented SCM in Orthopedic and Neurosurgery services at our institution (Ann Surg 2016;264(2):275-282). This model is innovative because the same Internal Medicine hospitalists are dedicated year round to the same surgical service. After the first year of implementing SCM, we conducted a propensity score weighted study with 17,057 discharges in the pre-SCM group (January 2009 to July 2012) and 5,533 discharges in the post-SCM group (September 2012 to September 2013) (Ann Surg 2016;264(2):275-282). In this study, SCM was associated with a decrease in medical complications, length of stay (LOS), medical consultations, 30-day readmissions, and cost.
Purpose: Since SCM requires ongoing investment by institutions, we now report a follow-up study to explore if there were continued improvements in patient outcomes with SCM. In this study, we evaluate if there was a decrease in medical complications, LOS, number of medical consultations, rapid response team calls, and code blues, and an increase in patient satisfaction with SCM in Orthopedic and Neurosurgery services between 2012 and 2018.
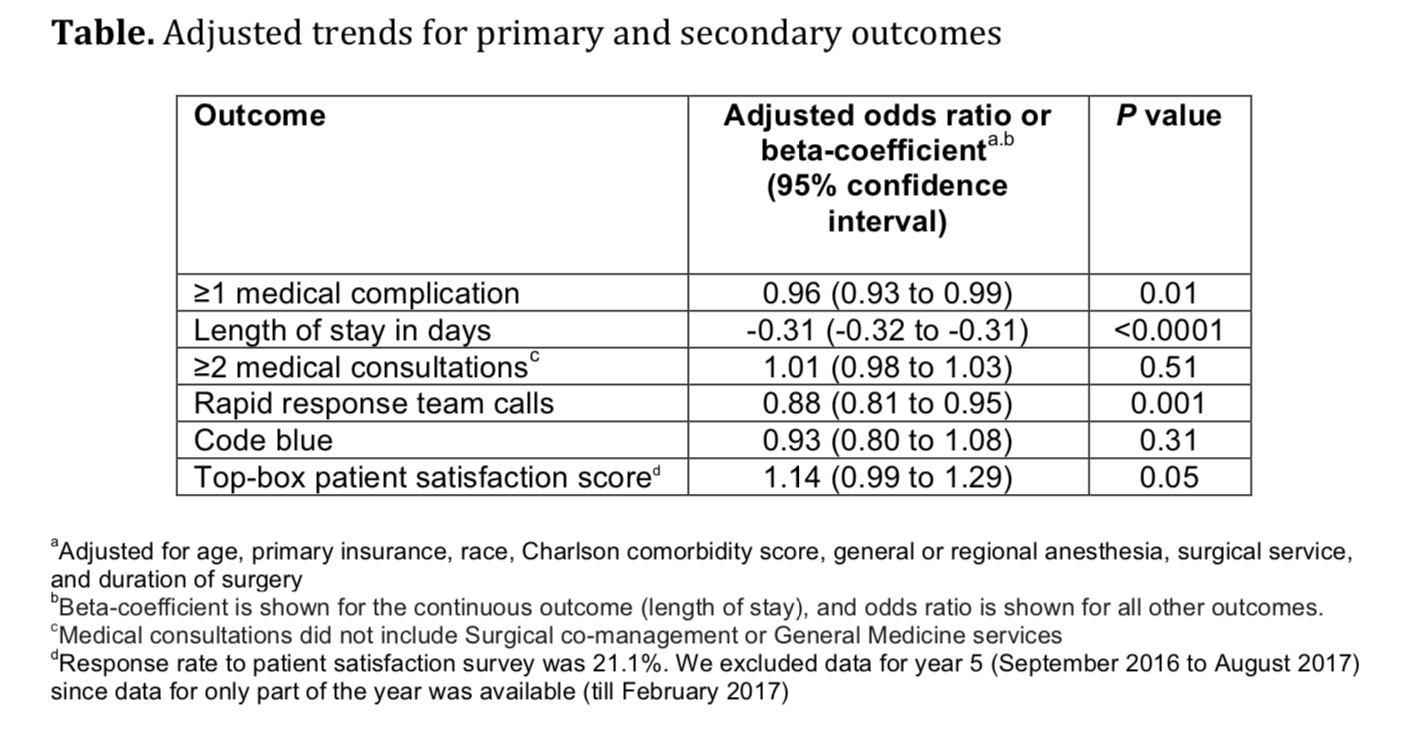
Description: We included 26,380 discharges from Orthopedic or Neurosurgery service between September 1, 2012 and June 30, 2018 at our academic medical center. We used regression analysis to assess trends in patient characteristics by year. Age, primary insurance, race, Charlson comorbidity score, general or regional anesthesia, surgical service, and duration of surgery were adjusted in regression analyses for outcomes.Results: 62.8% patients were discharged from Orthopedic surgery service. 72.5% patients underwent elective surgery and 88.8% received general anesthesia. Between 2012 and 2018, there was a significant increase in the median age of patients (from 60 years to 63 years), mean Charlson comorbidity score increased from 1.07 to 1.46, and median case mix index increased from 2.10 to 2.36. Comparing pre-SCM unadjusted rates reported in our prior study (January 2009 to July 2012) to post-SCM (September 2012 to June 2018), patients with ≥1 medical complication decreased from 10.1% to 6.1%, LOS (mean ± standard deviation) changed from 5.4 ± 2.2 days to 4.6 ± 5.8 days, patients with ≥2 medical consultations decreased from 19.4% to 9.2%, rapid response team calls changed from 1% to 0.9%, code blues changed from 0.3% to 0.2%, and patients with top-box patient satisfaction score changed from 86.4% to 94.2%.In the adjusted analysis, between 2012 and 2018, the odds of patients with ≥1 medical complication decreased by 3.8% per year (P = 0.0129), estimated LOS decreased by 0.3 days per year (P<0.001), and the odds of rapid response team calls decreased by 12.2% per year (P = 0.001). Changes over time in the odds of patients with ≥2 medical consultations, code blues, or top-box patient satisfaction score were not statistically significant. Based on the LOS reduction pre to post SCM, there were estimated average direct cost savings of $3424 per discharge between 2012 and 2018.
Conclusions: Since the implementation of SCM on Orthopedic and Neurosurgery services at our institution, there was a decrease in medical complications, LOS, and rapid response team calls. To our knowledge, this is one of the largest studies evaluating the benefits of SCM over 5.8 years.