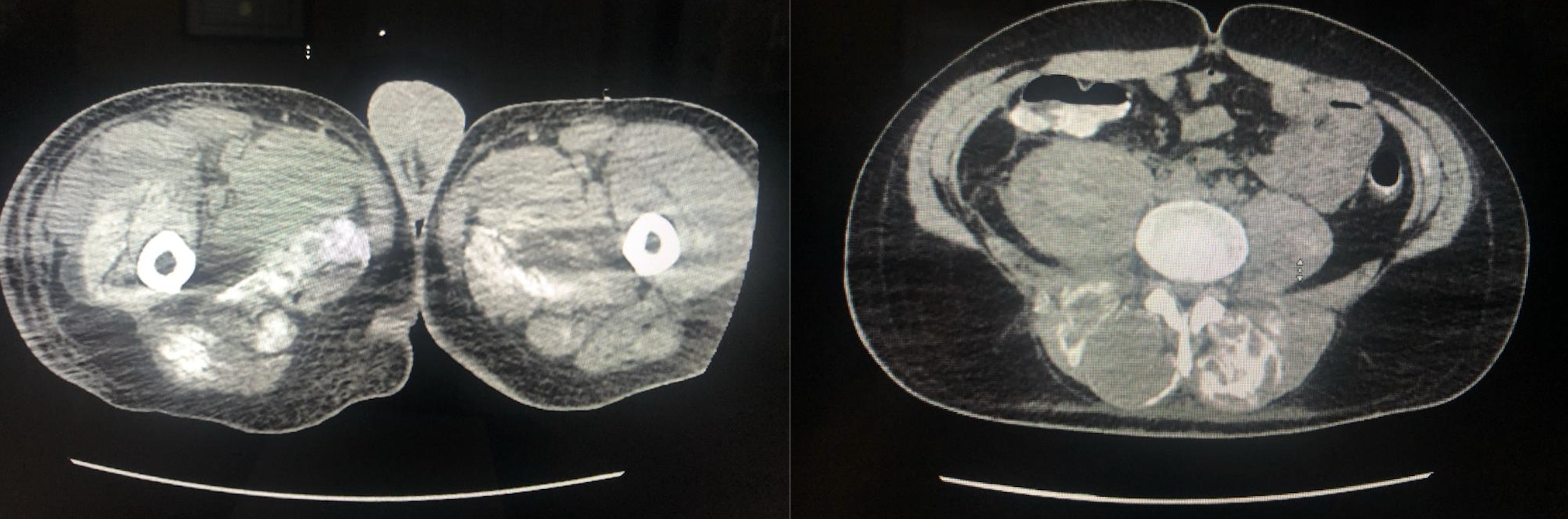
Case Presentation: A 26-year-old male with no significant past medical history was intubated due to respiratory failure from cocaine and fentanyl overdose. Admission labs showed severe rhabdomyolysis (creatinine kinase> 22K U/L), hyperphosphatemia (>20mg/dL) and hyperkalemia (>10mmol/L) with creatinine 2.9mg/dL. ICU course was complicated by hypoalbuminemia, chronic hypocalcemia (corrected calcium-7.6-8.4 mmol/L) and chronic hyperphosphatemia (5.6-10mg/dL). He received IV calcium daily for the first 3 weeks of his ICU stay until corrected calcium was normalized. He also developed sepsis, internal jugular vein thromboses and acute kidney injury treated with hemodialysis (HD). CT abdomen done sixteen days after admission showed multiple calcifications in the muscles of the chest, abdomen and pelvis consistent with Myositis Ossificans (MO). One month after admission he became severely hypercalcemic (corrected calcium >14mmol/L) needing further HD for several weeks. On examination he was noted to have calcifications within the muscles and soft tissues of his extremities that could be felt as hard solid lumps. He was discharged to acute rehab 10 weeks after admission.
Discussion: MO is a self-limiting, ossifying soft-tissue mass typically occurring within the skeletal muscles of young patients and most of the cases involve direct trauma to musculature(1)(2)(3). Non-traumatic etiologies like drug abuse, infection and neuromuscular dysfunction are less common(4)(5). The pathophysiology has been attributed to ‘endothelial-mesenchymal transition’ within muscle vasculature followed by differentiation of mesenchymal cells into osteoblasts and chondrocytes when exposed to inflammatory mediators(1). The development of MO in our patient is multifaceted. Cocaine induced rhabdomyolysis may have contributed to diffuse muscular micro-trauma and vasoconstriction causing ischemic tissue necrosis leading to intramuscular calcium deposition(6)(7). Critical illness neuro-myopathy and sepsis is also a consideration since our patient received paralytics which can mimic denervation injuries and create a microcosm that promotes MO development(4)(10).The relation between MO and rhabdomyolysis was described in a case by Bethoux et al(8). Calcium deposition within myocytes is thought to occur during the hypocalcemic phase of rhabdomyolysis, which in our patient was further compounded by administration of calcium in the setting of renal failure and hyperphosphatemia(8)(9). The hypercalcemia noticed later in our patient was due to calcium mobilization from diffuse calcifications. This systemic MO in our patient is unique because most cases are localized to the injured muscle. Such multi-systemic involvement has only been reported in the congenital form of the disease and in a patient with traumatic MO after sustaining diffuse bodily injury in an accident(11).
Conclusions: Systemic MO is a rare condition. Prolonged aggressive IV calcium repletion in patients with hyperphosphatemia without symptoms of hypocalcemia can lead to systemic MO. Monitoring the corrected calcium for hypoalbuminemia is imperative in the treatment of hypocalcemia.