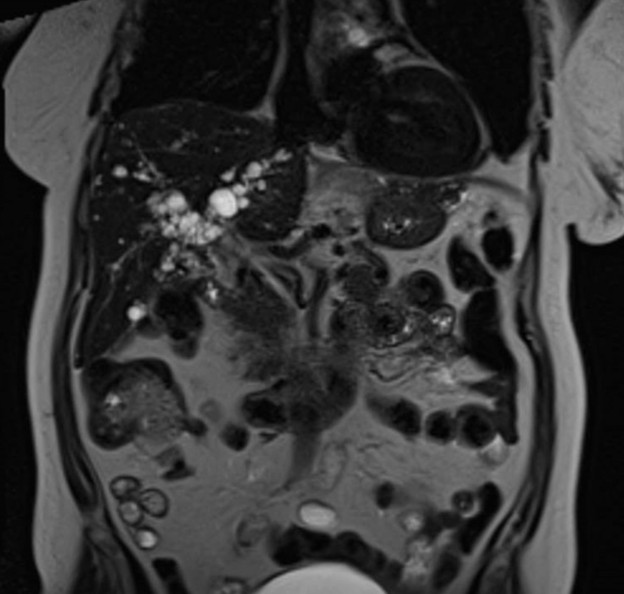
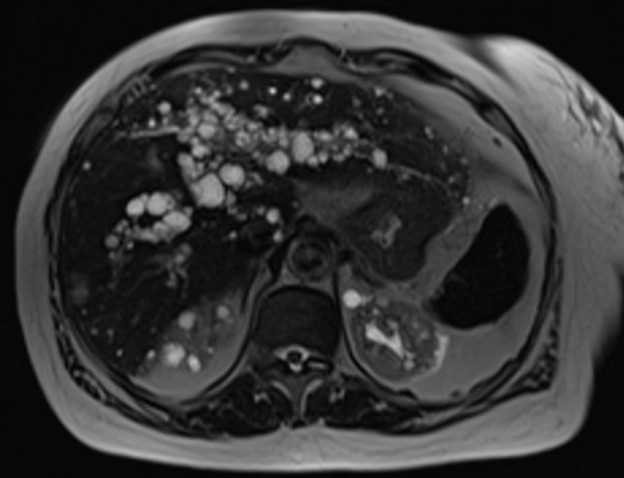
Case Presentation: The patient is a 69-year-old female with hemoglobin S/C disease, hypertension, and chronic kidney disease who presented to the hospital for lower back pain in the setting of a fall. CT scan demonstrated an L1 compression fracture and an incidental finding of cystic lesions in the liver and kidneys. Subsequent MRI demonstrated innumerable cysts in the kidneys and liver (Figure 1) following an intrahepatic biliary pattern. Admission labs were significant for a creatinine of 2.34 (eGFR of 22 mL/min/1.73m2) and no derangements of LFTs. Patient was diagnosed with incidental Caroli’s disease, likely in the setting of autosomal dominant polycystic kidney disease (ADPKD). The patient denies ever having had symptoms of jaundice, RUQ pain, or cholecystitis or cholangitis. Although she was told she had chronic kidney disease in the past, the cause was never elucidated.
Discussion: Caroli’s disease presents with cystic dilation of intrahepatic bile ducts with the absence of cirrhosis or portal hypertension [1]. The incidence is thought to be 1 in 1,000,000 and generally presents before the age of 30 [2]. It is diagnosed primarily through imaging studies, such as CT, MRI, ERCP, and MRCP, and requires that the cysts be present within the biliary tree [3]. Imaging features are a “string of beads” appearance on MRI [4], and the central dot sign seen on CT imaging, representing portal vasculature within a pseudoaneurysm [4,5]. Polycystic liver disease differs from Caroli’s disease in that the cysts of PLD rarely involve the bile ducts.Due to the biliary ectasia, Caroli’s disease can be associated with cholelithiasis, cholangitis, and hepatic abscesses, resulting in biliary colic, jaundice, or pancreatitis [1,2,6,7,8]. However, similar to this case, it may remain asymptomatic throughout life [2,4,9].When Caroli’s disease is associated with hepatic fibrosis it is considered Caroli’s syndrome [1,5,6]. Caroli’s syndrome occurs more frequently than Caroli’s disease [5]. Caroli’s syndrome is often associated with ARPKD and as such primarily presents in children [1,4,6,10]. ADPKD affects patients later in life than ARPKD and is a milder form of the disease [11] and is likely the source of kidney disease in our patient. Cystic liver disease is common in ADPKD, occurring in upwards of 75%-90% of cases, but is usually polycystic liver disease instead of Caroli’s disease [12]. Only a few case reports have demonstrated Caroli’s disease with ADPKD [1,8,10].
Conclusions: In conclusion, although Caroli’s disease is rare, patients with this condition are at risk of developing biliary complications and is associated with cystic kidney disease. Given this condition’s association with cystic kidney disease, when conducting renal ultrasound studies, if cystic lesions are found concerning for ADPKD then examination of the liver should also be considered. Finally, this case illustrates a situation where the patient’s kidney disease was likely attributed to her hypertension when in fact her ADPKD was the likely contributor. This underscores the importance of comprehensive transitions of care with outpatient specialist, particularly in light of this incidental finding.