Background: Providing patient centered care is a core value of all healthcare systems in our nation. However, having a code status discussion with patients and their families continues to be a challenging endeavor due to multiple factors such as competing priorities and time constraints, especially in the hospital setting. To improve code status discussion and documentation, Hospitalists at Lehigh Valley Health Network (LVHN) received comprehensive education about the importance of code status discussion and the skills to lead those crucial conversations. A predictive model was then utilized to identify high-risk patients, as defined by the End-of-Life (EOL) Care Index and Inpatient Deterioration Index (IDI), to guide an electronic Best Practice Advisory (BPA) alerting clinicians for the need of code status discussion. Using education, transparent data sharing, accountability, and incentive, we successfully improved and maintained code status discussion and documentation compliance.
Purpose: To improve compliance with code status discussion and documentation in high-risk patients to improve patient-centered care.
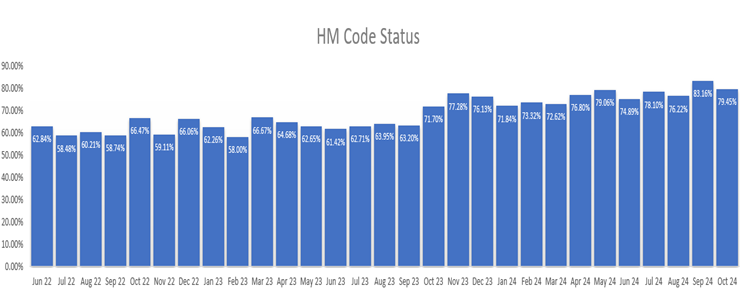
Description: The EOL Care Index is a logistic regression that predicts the risk of one-year mortality. It uses 3 demographic, 2 lab, 26 comorbidity, and 15 active medication variables to make predictions among adults (≥18 years old) with one in-person ambulatory visit and one separate ED visit, hospitalization, or in-person ambulatory visit ≤ 2 years prior to prediction (High risk is > 30, Positive predictive value is 16%, and C-statistic is 0.91).The IDI is an ordinal, logistic regression model that predicts transfer to ICU, rapid response, code blue, or mortality within the next 38 hours. The model uses age, vital signs, 4 nursing assessment, and 7 lab variables. The population is a patient class of Inpatient or Observation, ≥ 18 years old during encounter, bedded ≥ 2 hours before discharge, and primary diagnosis is not related to pregnancy or mental illness (High risk is > 55, positive predictive value is 55%, and C-statistic is 0.79).At LVHN, a large care system with over 327000 annual ED visits and 75000 annual acute admissions in eastern PA, those two scores were used to generate a BPA that fires to recommend code status discussion with patients for whom no discussion is documented and have high-risk IDI or EOL indices. The BPA includes a direct link to the appropriate Epic documentation tool for clinicians. This BPA fired from 7am-7pm to avoid overwhelming Nocturnists and decrease alarm fatigue. By combining these tools with education, transparent data sharing, accountability, and incentives, Hospitalists improved code status discussion to 70-80% in high-risk patients, as compared baseline coverage of 50-60% for all patients. This resulted in a drastic increase in overall institutional code status discussion, documentation, DNR status, and ICU transfers.
Conclusions: Using predictive analytics to direct Hospitalists to appropriate patients with high risk for one year mortality was successful in improving code status discussion and documentation compliance. Our predictive model offers the advantage of creating an efficient and high yield reminder to address goal of care for high-risk patients while minimizing alert fatigue by avoiding warning for those with low risk, thereby improving care. Future projects will use this model to drive better goal-directed interventions oriented on patient care.