Background: Peripherally intravenous (PIV) vascular access is important for the care of hospitalized children and one of the most common, and difficult, procedures performed in the hospital. For many reasons, especially in pediatrics, there is often difficulty obtaining or maintaining reliable vascular access in hospitalized children, leading to patient and parental distress and care delays. Unfortunately, sometimes pediatric patients with difficult intravenous access (DIVA) require central venous catheter (CVC) placement for reliable vascular access. At our institution, feedback from providers on the pediatric acute floors revealed concerns about delays in care and inappropriate central line use for patients with DIVA due to non-standardized vascular access processes. We recognized an opportunity to advocate for increased utilization of ultrasound-guided PIVs (USGPIV), which ideally should be standard of care for pediatric patients. However, limited procedural expertise and lack of appropriate resources often limited making this an easily accessible procedure for patients. Through better identification of patients at risk for DIVA, processes could be optimized to allocate limited USGPIV resources to this vulnerable cohort.Our primary aim was to increase the utilization of USGPIVs for pediatric patients with a documented high DIVA score (≥4) admitted to a single acute care unit of our Children’s hospital composed of predominantly general pediatric and pediatric surgery patients (age < 18).
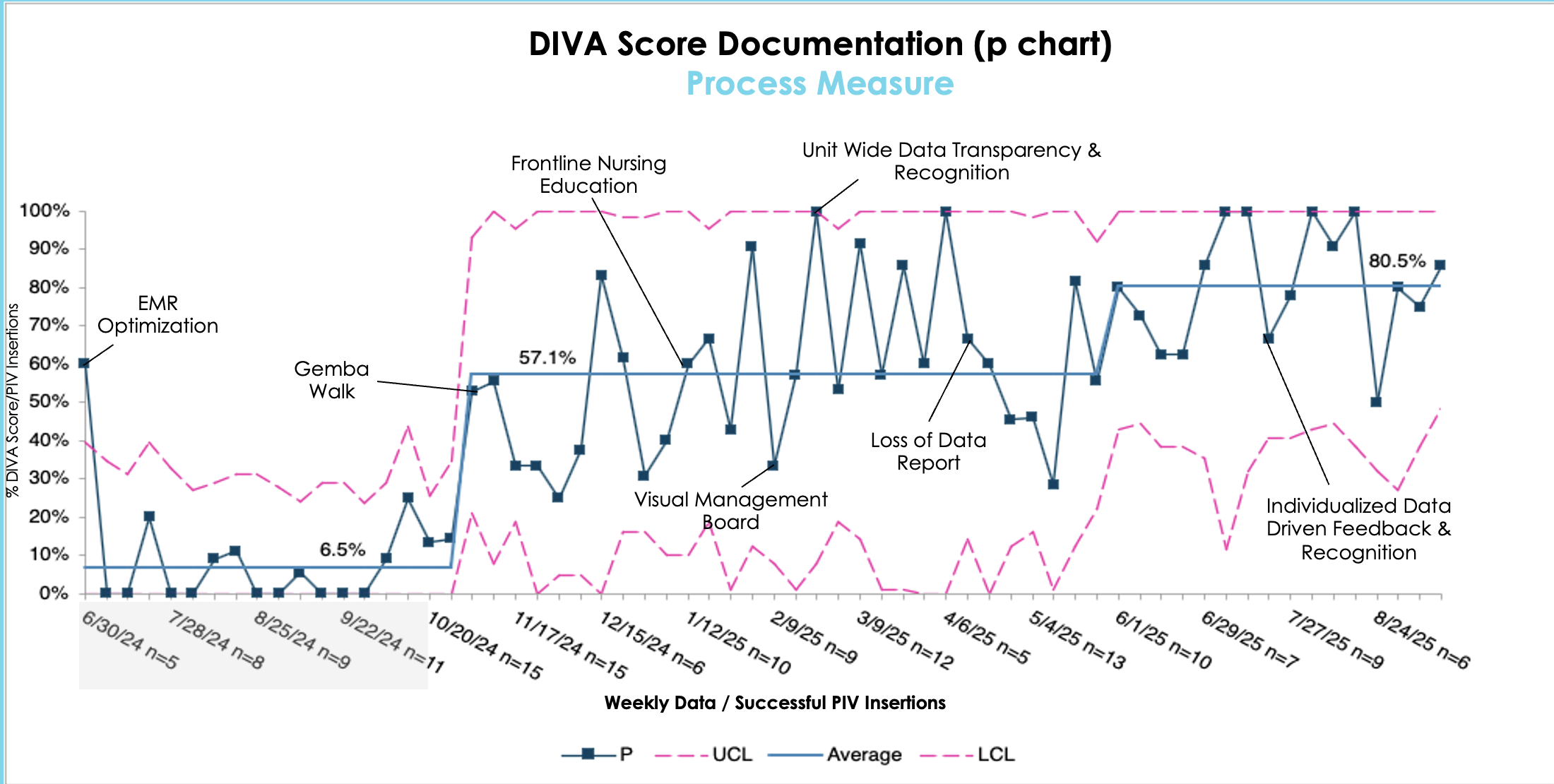
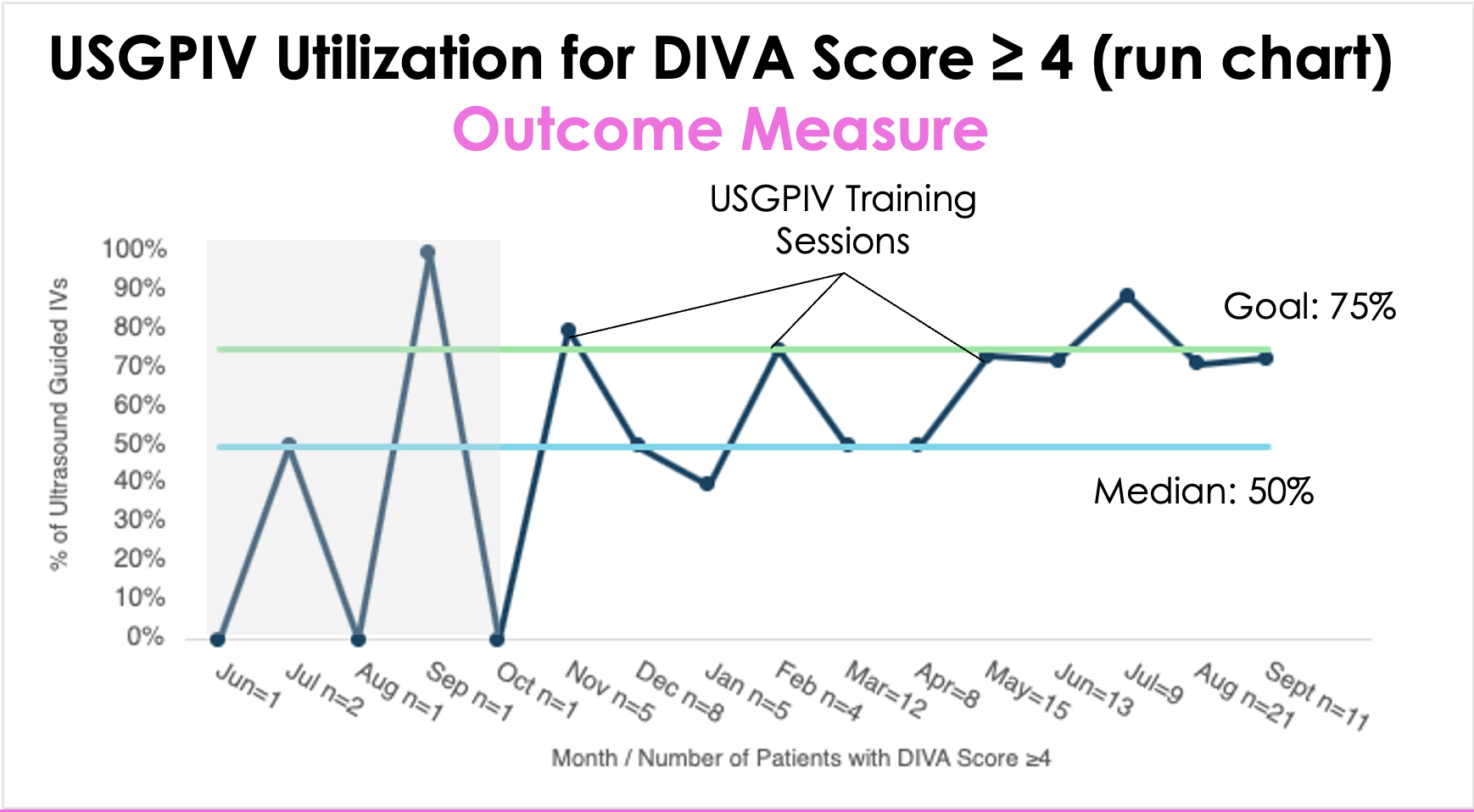
Methods: Prior to our interventions, with input from the expertise of our project team, a new pediatric vascular access pathway was created. The new process began with the bedside nurse obtaining and documenting a DIVA score for any patient who needed a new PIV. A high DIVA score prompted escalation of care and interventions, including the use of ultrasound.A multidisciplinary team was established and root cause analysis and process mapping were performed. A key driver diagram was used to identify interventions for improvement cycles. Key quality improvement (QI) interventions included incorporating DIVA score documentation into the electronic medical record (EMR), nursing education, visual management boards, USGPIV training sessions, and data driven feedback. We collected data from June 2024 to September 2025. To assess the impact of our improvement efforts and support rapid-cycle learning, biweekly data was reviewed throughout the project period. Our primary process measure was the percentage of DIVA scores documented per patients with a successful PIV insertion attempt on a single-floor of our Children’s hospital. Our primary outcome measure was utilization of ultrasound in patients with a documented high DIVA score.
Results: Through our QI interventions, we increased the use of DIVA score documentation (6.5% to 80%), improved other aspects of PIV documentation including accuracy of PIV attempts, increased USGPIV utilization for all patients, and specifically improved access to USGPIV procedures for our high DIVA score patients (33.3% to 75%).
Conclusions: We improved identification of patients at risk for DIVA through implementation of a DIVA scoring system and strategically allocated limited resources for ultrasound-guided peripheral vascular access procedures to this at-risk cohort. Next steps include measuring improvements in care delay reduction and avoiding unnecessary central line placement for patients with DIVA.