Background: Faculty development (FD) programs increase faculty engagement, retention, work satisfaction, and collective success, but many hospitalist groups struggle with implementing FD programs due to limited time, lack of support for faculty participation, and curricula that often do not align with faculty priorities. A recent qualitative study exploring FD from 17 academic hospital medicine programs found less than half had established FD programs.
Purpose: To implement a FD program within a Division of Hospital Medicine (DHM) that addressed common implementation barriers and fostered a community of practice, while focusing on cognitive load theory to maximize learning.
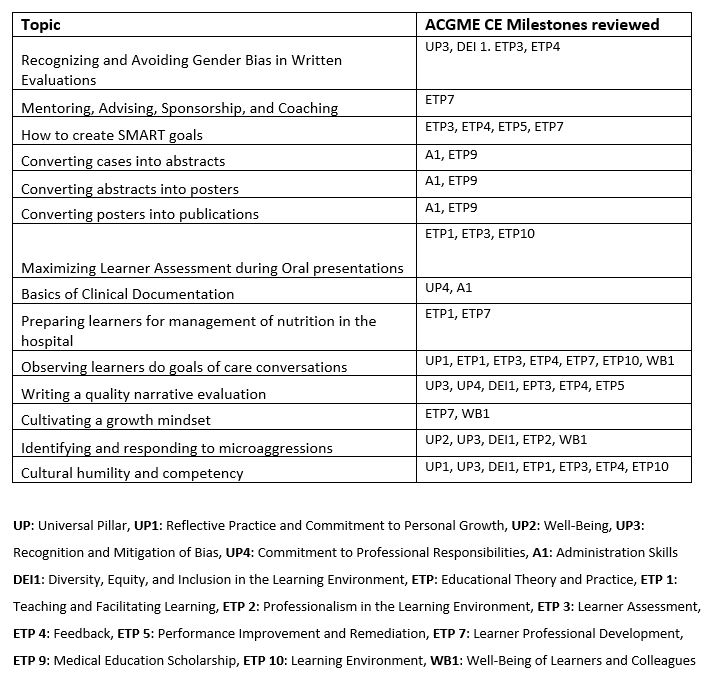
Description: The DHM at the Veterans Affairs Greater Los Angeles Health Care System, a teaching affiliate of UCLA, includes 25 full-time faculty hospitalists. To address common implementation barriers, we developed a FD curriculum that fit into monthly division meetings using bite-sized teaching (BST) delivered by peer faculty to develop shared clinician educator (CE) skills. We began the Hospitalist Faculty Development (HFD) pilot in November 2022. CE topics were presented by peer hospitalists using the ACGME CE Milestones as a framework. Topics started with clear learning objectives and finished within 10 minutes via the BST approach using brief, focused learning units. The HFD program was offered to all DHM faculty during monthly DHM meetings. Table 1 includes a list of topics presented during the pilot. An asynchronous learning option was also available. Presenters were self-selected based on interest and were provided feedback before and after each session. Teaching in the curriculum was included in annual performance pay criteria for faculty.We sent confidential, anonymous surveys to all members of the DHM. We used a modified Kirkpatrick model as a framework to generate questions. The authors were excluded from the survey. This study was exempt by the UCLA Institutional Review Board. Of the 21 hospitalists surveyed, 17 completed the survey (81% response rate). Sessions were well attended with most attending 6 or more of the 14 meetings. All respondents agreed or strongly agreed it is important to advance their CE skills. Nearly all (94%) felt they learned something valuable and were satisfied with the quality of teaching, and 88% were satisfied with the short format and variety of topics. A few comments suggested providing more time to promote discussion.75% reported they changed their practice or directly applied new skills. Examples were avoiding biased language in narrative evaluations of learners, incorporating new phrases in managing microaggressions, and improved skills with preparing posters and abstracts. About a third used the supplemental materials (handouts, articles, slides, and recorded videos) themselves and to share with other learners. Presenters (n=9) agreed that participation improved their ability to teach and fostered a sense of community.
Conclusions: Introducing longitudinal peer faculty teaching using a BST format during monthly DHM meetings was feasible, well-liked, and resulted in self-reported change in practice. By addressing time constraints and lack of engagement, the HFD program could be adopted within busy academic hospitalist groups.