Background: Hospital throughput and early discharges are of high priority to health systems. However, busy hospitalists may have multiple competing priorities that delay timely completion of discharge tasks. We evaluated the effect on discharge timing of providing a clinical assistant to help hospitalists with discharge tasks.
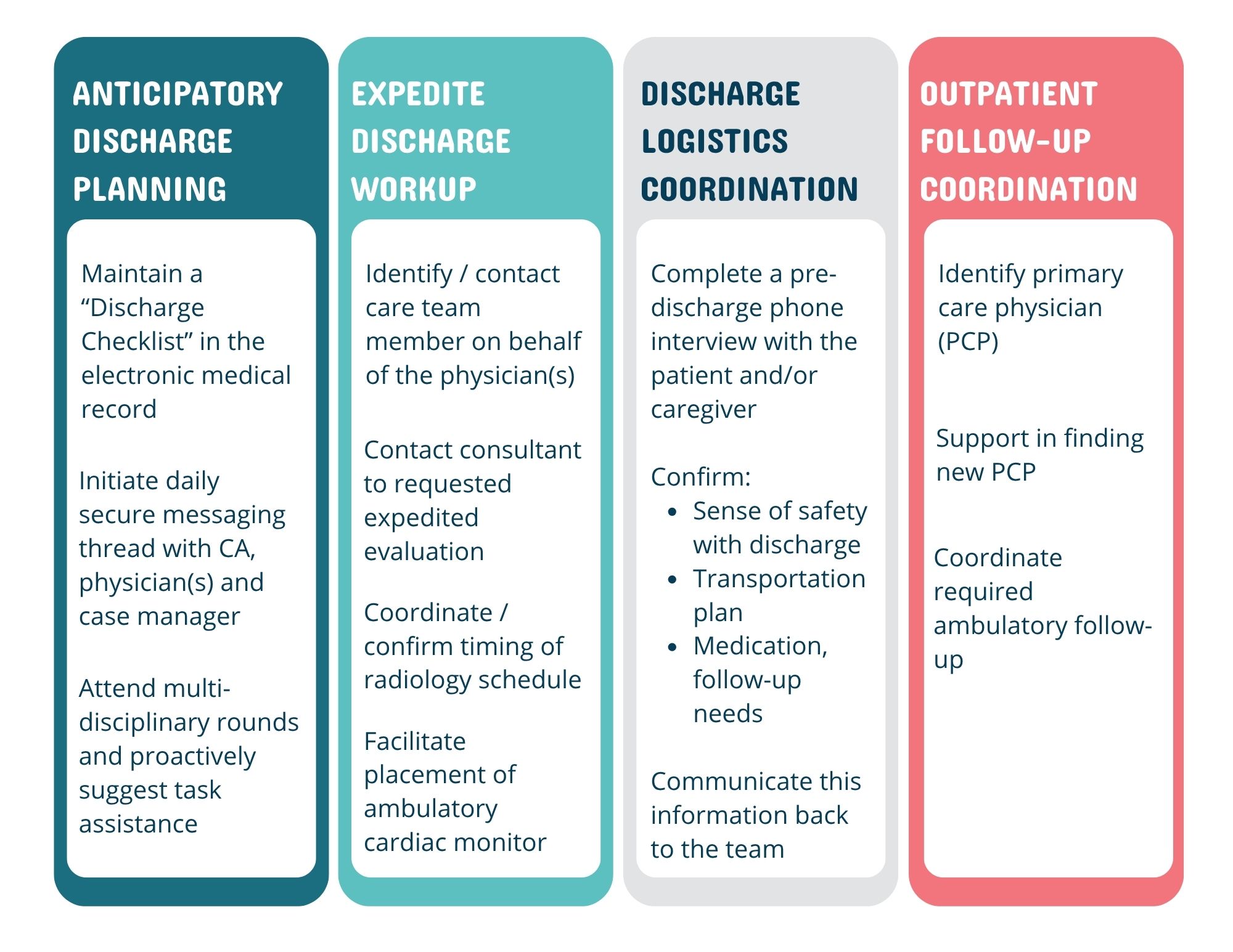
Methods: This prospective interventional study was conducted over a 3-week period (March 18-April 10, 2025) on the general medicine service of a 600-bed academic teaching hospital that has both direct care hospitalists (working without advanced practice providers) and teaching teams (hospitalists working with residents and medical students). The intervention comprised a clinical assistant who proactively screened for pending discharges and helped teams complete discharge-related tasks (Figure 1). Four direct care hospitalist teams and 4 teaching teams were given access to the clinical assistant intervention. A control group of 5 direct care and 4 teaching teams had access to usual hospital discharge workflows. Study outcomes were percent discharge orders by 10 am, median time of actual discharge, and length of stay (LOS). We also surveyed hospitalists in the intervention arm to assess their experience working with the clinical assistance.
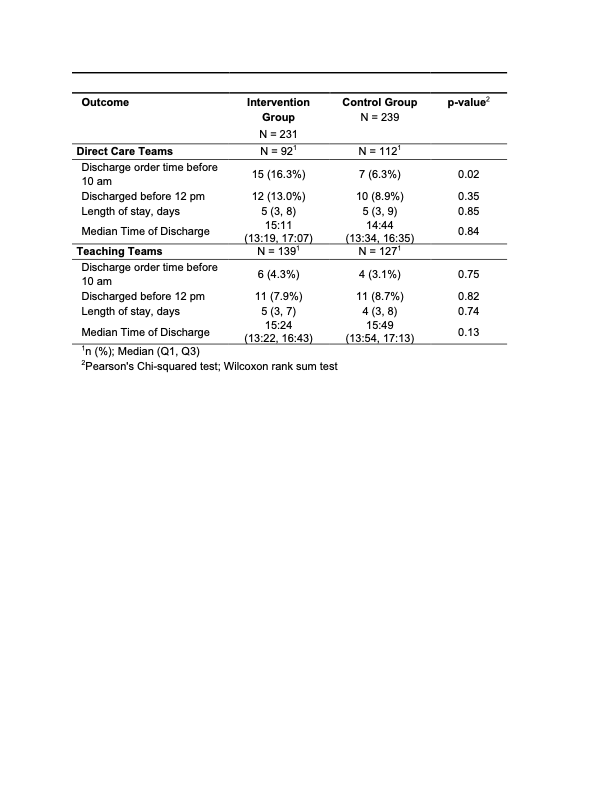
Results: There were 239 patient discharges in the intervention arm and 231 discharges in the control arm. In the direct care teams, the intervention arm had a higher proportion of discharge orders signed by 10am (16.3% vs 6.3%, p= 0.02) but there was no statistically significant difference in the teaching teams (Table 1). The actual time patients left the hospital showed no statistically significant difference between direct care intervention and control arms (15:11 vs 14:33, p=0.84). When we surveyed hospitalists exposed to the intervention, satisfaction with the discharge process increased from 18% to 52% (n=31 respondents, 60% survey completion).
Conclusions: Discharge support from a clinical assistant significantly increased the proportion of discharge by 10am orders and satisfaction with the discharge process among direct care hospitalists. Enhanced discharge support did not affect the actual time of discharge, suggesting that the discharge process involves a more complex interplay of factors.