Background: Congestive heart failure (CHF) is a leading cause of hospital readmissions, posing significant challenges to both patient outcomes and healthcare expenditures. Medicare data indicates that approximately 25% of patients admitted with a CHF exacerbation are readmitted within 30 days, underscoring the need for improved care strategies. Previous studies have demonstrated that structured discharge planning and patient education reduce hospital readmissions among CHF patients.At NYU Langone – Brooklyn, we implemented a cohorting model on unit LB4500, grouping cardiology patients together to deliver focused, multidisciplinary care. There is limited evidence on whether cohorting patients to a dedicated unit enhances any outcomes. This study aims to evaluate the impact of cohorting on 30-day readmission rates for CHF patients.
Methods: This study performed a retrospective chart review of NYU Langone – Brooklyn inpatient admissions occurring from September 2024 to April 2025. The analysis compared two cohorts: patients initially admitted to unit LB 4500 and those admitted to other units at the same hospital. To ensure a relevant population, the review excluded ICU patients, patients with ESRD, and those whose length of stay exceeded 30 days. The study’s focus was the rate of 30-day readmission to any facility within the NYU Langone Health system. Additionally, average length of stay was reviewed as a secondary outcome.
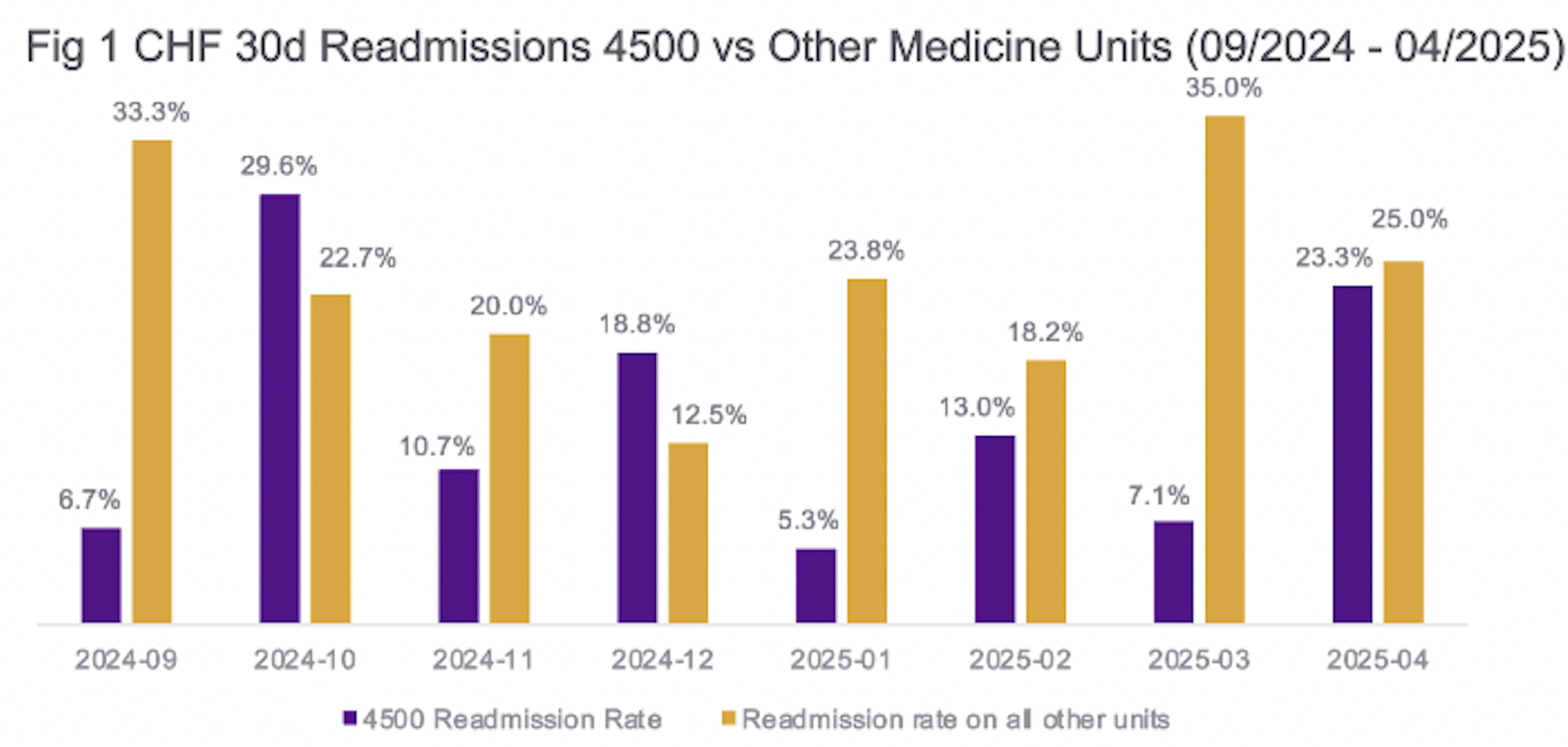
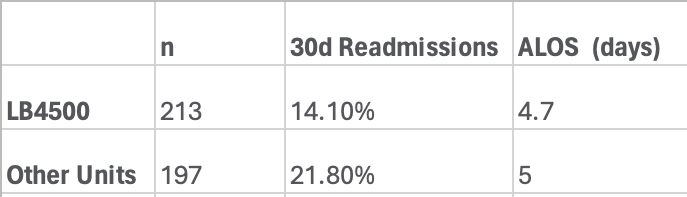
Results: A retrospective analysis of Congestive Heart Failure (CHF) patients admitted to NYU Langone – Brooklyn between September 2024 and April 2025 compared outcomes based on initial admission to Unit LB4500 versus other medicine units. Of the 410 total patients analyzed, 213 were admitted to LB4500 and 197 to other units. The data revealed that the cohorted Unit LB4500 had a lower average 30-day readmission rate at 14.1%, compared to 21.8% for patients admitted to other medicine units. Additionally, patients on Unit LB4500 experienced a slightly shorter average length of stay (LOS), averaging 4.7 days compared to 5.0 days for patients in the rest of the hospital.
Conclusions: This retrospective analysis found that patients admitted to a cohorted cardiology unit experienced a lower 30-day readmission rate despite having an also shorter average length of stay. These findings suggest that cohorting patients and providing specialized, targeted care for this population could be an effective strategy for improving one of the most challenging metrics in healthcare.The reduced readmission rate for patients on LB4500 can likely be attributed to several key features of a cohorted unit. By dedicating a unit specifically to CHF patients, the care team can focus on the unique and complex needs of this population. The interdisciplinary approach on LB4500 plays a crucial role in delivering tailored care that patients might not receive on general medicine units. From more closely monitored fluid intake and output and daily weight tracking by nurses, to enhanced post-discharge support through community health workers and home care services, these focused interventions likely contribute to the improved outcomes. Additionally, the closer collaboration between the primary care team and the advanced heart failure consulting team further strengthens care continuity and helps prevent readmissions. While the specific factors that contribute most to these improved outcomes remain unclear, further investigation is needed to identify which variables are most effective in reducing readmissions.