Background: Missed diagnoses in clinical documentation leads to increased coding queries for providers, skews crucial quality metrics such as mortality and readmission indices, and ultimately has significant financial and reputational impacts for hospitals. A substantial opportunity exists to improve documentation precision to accurately capture diagnoses that reflect severity of patient illness and complexity upon admission. Current documentation practices are often burdensome, time-consuming, and yield widely variable information depending on provider expertise and understanding of coding specificity.
Purpose: At our quaternary care academic medical center, we leveraged our hospital’s PHI-encrypted Artificial Intelligence (AI) tool to create a specific task that generates and standardizes discharge summaries, enhances the capture of diagnoses present on admission, and provide this information for each patient within a minute. The primary goals were to reduce the time physicians and APPs spend on discharge paperwork, improve the capture of Comorbidities and Complications (CCs) and Major Comorbidities and Complications (MCCs) to more accurately reflect and improve Case Mix Index (CMI), and ultimately free up provider time for direct patient care. This initiative also aimed to improve the capture rate of hospital diagnoses, thereby ultimately impacting hospital reimbursement and quality metrics. To assess provider perception and impact on workflow, a survey was sent to hospital medicine providers (residents, attendings, NPs, and PAs) both before and after the Discharge AI tool’s implementation.
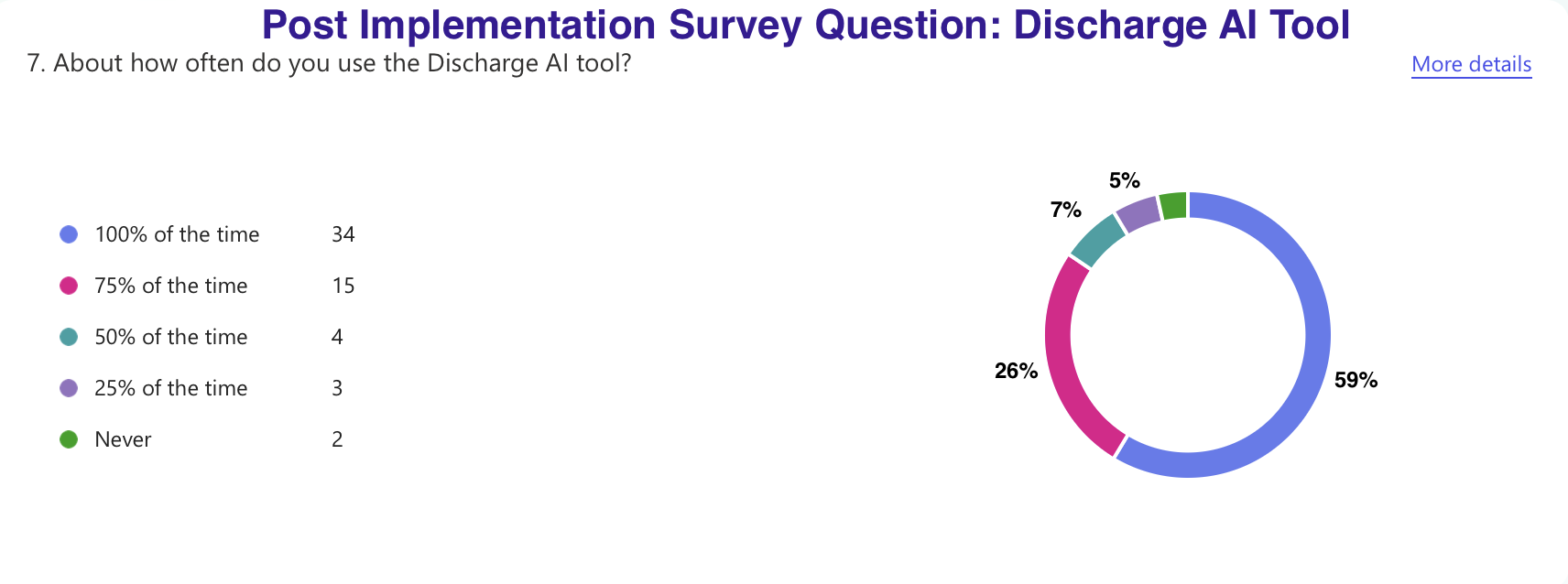
Description: A need was identified to improve the capture rate of commonly missed diagnoses, such as electrolyte imbalances (acidosis, alkalosis, hypokalemia, hyperkalemia), which significantly impacted hospital metrics and reimbursement. Concurrently, there was a need to standardize discharge documentation, as providers were already utilizing AI in varied ways. A pre-implementation survey of 46 providers revealed that the majority found discharge paperwork time-consuming and that documentation burden reduced their direct patient care time. Provider comfort with digital tools varied: 25% had no AI experience, 41% minimal, and 33% moderate (used it regularly). Post-implementation, nearly all 58 participants reported that the Discharge AI tool reduced time spent on paperwork, improved documentation specificity and accuracy, saved daily time, facilitated earlier patient discharges, and enhanced their wellbeing. Regarding coder queries, 48% reported receiving fewer, while 48% noted no change. Notably, 84% of providers were using the new Discharge tool at least 75-100% of the time. Since its roll-out in October 2025, preliminary data demonstrates a 56% increase in the capture rate of electrolyte imbalance diagnoses within the hospitalist group (CCs including acidosis increased by 81%, hypocalcemia by 173%, and hyponatremia by 27%).
Conclusions: The strategic and responsible use of AI in discharge documentation has the potential to significantly improve provider efficiency, reduce burnout, and enhance the accurate capture of diagnoses for coding purposes. Future iterations of the tool will incorporate survey feedback, expand to other departments, and continue to monitor for sustained positive outcomes. Crucially, human oversight to vet the accuracy of AI generated content remains important to ensure quality documentation.
.png)