Background: Many hospitals set targets for discharging patients before noon in efforts to optimize patient throughput. However, discharge before noon (DCBN) has been associated with increased length of stay (LOS) in an adult population. The relationship between discharge time of day and LOS in pediatric patients is uncertain. This study aims to evaluate the relationship between DCBN and LOS in pediatric patients.
Methods: We conducted a retrospective analysis of pediatric medical and surgical discharges from a single academic medical center from May 2014 through March 2017. LOS was defined as discharge date and time minus admission date and time. DCBN was defined as a discharge after 8:00am and before noon. Newborns, patients that died, and patients with LOS less than two days or greater than two standard deviations from the discharge service’s mean LOS were excluded.
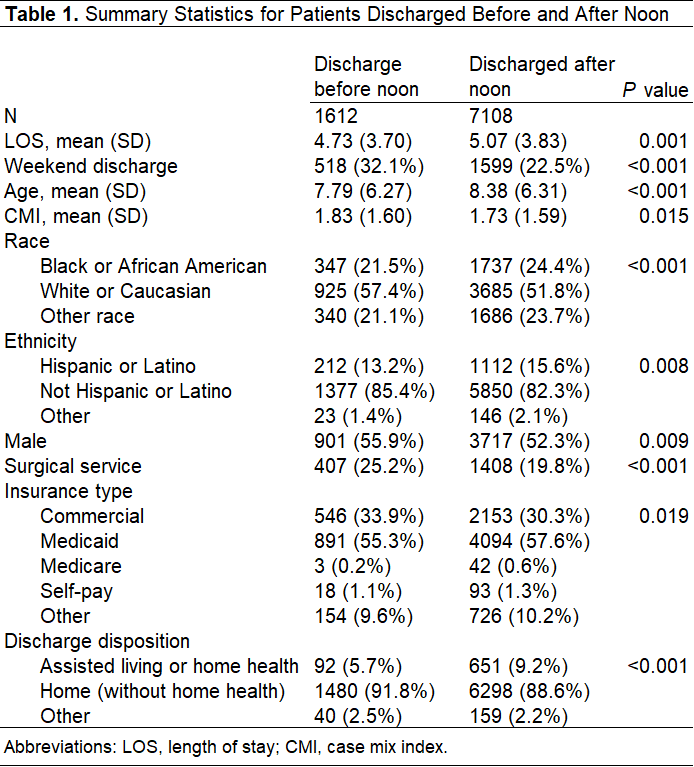
We used t-tests and χ2 tests to compare baseline demographic and clinical characteristics of DCBN. Multivariate ordinary least squares models were used to evaluate the association between DCBN and LOS. After running an unadjusted model, we included covariates that correlated with DCBN at P < .05 and the covariate sex for reasons of face validity and clustered on discharge attending to adjust standard errors. All covariates are given in Table 1. Our institutional review board approved this study.
Results: A total of 8,720 unique patient encounters were included in the study. We observed 1,612 discharges before noon and 7,108 discharges after noon with a median LOS of 3.88 and a median case mix index (CMI) of 1.19. The characteristics of the patient encounters discharged before and after noon are shown in Table 1.
DCBN was associated with a .23 day shorter LOS as compared to discharge after noon (P=.019) when controlling for age, sex, race, ethnicity, surgical discharge service, weekend discharge, CMI, insurance type, and discharge disposition. Surgical and weekend discharges were associated with a 1.5 and .7 day decrease in LOS, respectively, both significant at P <.001. CMI and Medicaid insurance type were associated with a .82 and .4 day increase in LOS respectively, both significant at P <.001.
Conclusions: Children with DCBN in our institution had a shorter LOS when controlling for other factors associated with LOS. This finding contradicts data from adult patients suggesting that DCBN was associated with longer LOS. Associations of DCBN and LOS in different patient populations and causal relationships should be explored to optimize patient flow and hospital utilization.